Abstract
Objectives:
Stereotactic body radiotherapy (SBRT) is an evolving treatment for the local management of pancreatic cancer (PC). SBRT is offered as an adjuvant therapy for non-operative patients or for salvaging local failure. The main purpose of this study is to report our initial experience in terms of local control (LC) and toxicity for PC patients treated with SBRT.
Methods & Materials:
We conducted a retrospective review of patients treated with SBRT. Patients were identified after a multidisciplinary rounds discussion. Treatment was delivered on Truebeam using abdominal compression (AC) or end expiratory breath hold (EEBH) technique for motion management with image guidance using implanted fiducial markers. Target delineation was done using departmental protocol & uniform Planning Target Volume (PTV) margin of 5mm was generated. The median prescribed dose was 35Gy (30-50Gy), delivered in 5 fractions. Toxicities were recorded using Common Terminology Criteria for Adverse Events (CTCAE) v5.0 during radiotherapy (RT) & at 3, 6, 9 and 12 months follow up. Survival were estimated using Kaplan-Meier method.
Results:
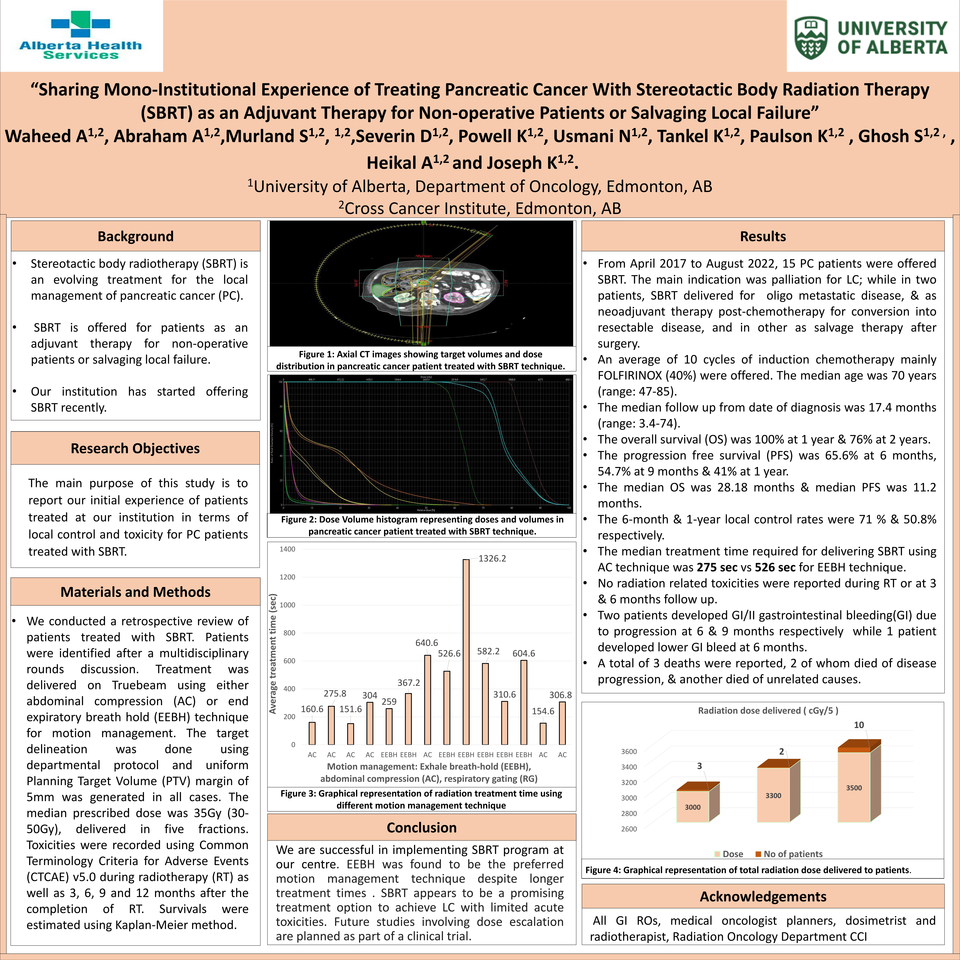
From April 2017 to August 2022, 15 PC patients were offered SBRT. The main indication was palliation for LC; while in two patients, SBRT delivered for oligo metastatic disease, & as neoadjuvant therapy post-chemotherapy for conversion into resectable disease, and in other as salvage therapy after surgery. An average of 10 cycles of induction chemotherapy mainly FOLFIRINOX (40%) were offered. The median age was 70 years (range: 47-85). The median follow up from date of diagnosis was 17.4 months (range: 3.4-74). The overall survival (OS) was 100% at 1 year & 76% at 2 years. The progression free survival (PFS) was 65.6% at 6 months, 54.7% at 9 months & 41% at 1 year. The median OS was 28.18 months & median PFS was 11.2 months. The 6-month & 1-year local control rates were 71 % & 50.8% respectively. The median treated target volumes were PTV;75.1 cm3, gross tumor volume;28.6 cm3 and internal target volume (ITV) ; 24.8 cm3. The median treatment time required for delivering SBRT using AC technique was 275 sec vs 526 sec for EEBH technique. No radiation related toxicities were reported during RT or at 3 & 6 months follow up. Two patients developed GI/II gastrointestinal bleeding(GI) due to progression at 6 & 9 months respectively while 1 patient developed lower GI bleed at 6 months. A total of 3 deaths were reported, 2 of whom died of disease progression, & another died of unrelated causes.
Conclusion:
We are successful in implementing SBRT program at our centre. EEBH was found to be the preferred motion management technique despite longer treatment times . SBRT appears to be a promising treatment option to achieve LC with limited acute toxicities. Future studies involving dose escalation are planned as part of a clinical trial.



