Abstract
Introduction: The Wittmann Patch is a device used to bridge and approximate the opening of the abdominal wall, therefore preventing lateral retraction of the wall in cases in which repeat abdominal access is necessitated. This is traditionally approached using the step up approach, shown to decrease complications. This step up approach begins with antibiotic treatment, fluids- nonoperative, conservative management. In cases of necrotizing pancreatitis like ours in which the step-up approach is not feasible, the method of leaving the abdomen accessible can be vital in the patient’s overall clinical course. We present a unique case of usage of the Wittmann patch for abdominal closure of exploratory laparotomy to assist in clarifying this discrepancy. This report will show the importance of the device’s ease of application and abdominal entry, as well as counteraction of lateral retraction that was necessary for our patient’s successful result.
Case Description: A 31-year old male presented to the ER with severe epigastric pain radiating to the left upper quadrant, nausea, nonbilious emesis, decreased appetite, and fatigue. Our patient had a history of prediabetes, hypertension, and obesity. A CT scan showed hepatic steatosis as well as severe acute pancreatitis secondary to hypertriglyceridemia.
Three weeks later, our patient developed abdominal compartment syndrome and was taken for decompressive laparotomy. The procedures included diagnostic laparoscopy, exploratory laparotomy, cholecystectomy, and pancreatic necrosectomy. Intraoperatively, necrotizing pancreatitis and gangrenous gallbladder were found. Drains were placed and a temporary abdominal closure was achieved using cassette drape. Abdominal wash-out was repeated three more times to keep the patient stable.
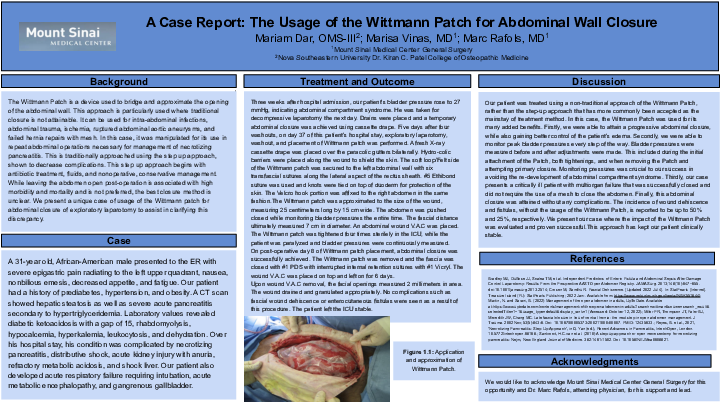
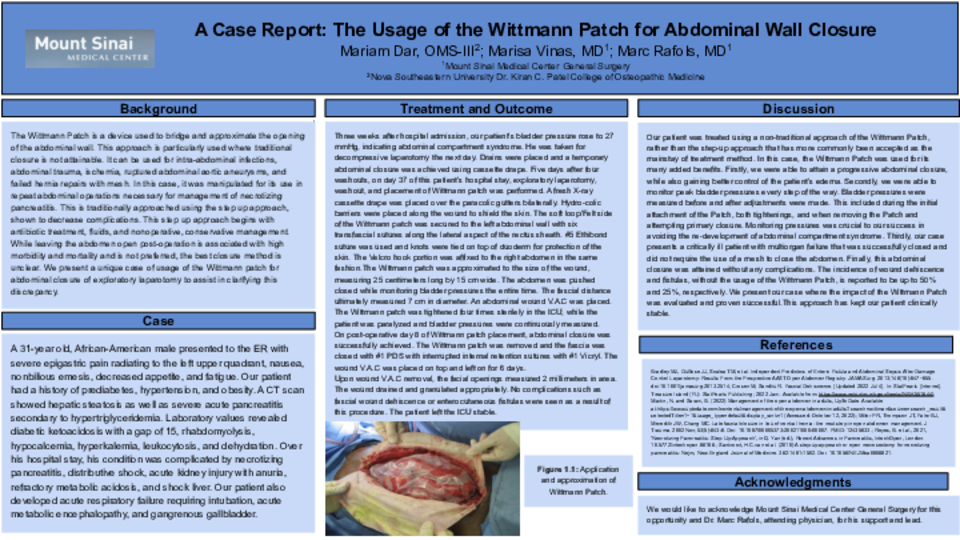
On day 37 of this patient’s hospital stay, exploratory laparotomy, wash out, and placement of Wittmann patch was performed. After wash-out to help bowel edema, a fresh X-ray cassette drape was placed over the paracolic gutters bilaterally. Hydro-colic barriers were placed along the wound to shield the skin. The soft loop/Felt side of the Wittmann patch was secured to the left abdominal wall with six transfascial sutures along the lateral aspect of the rectus sheath. #5 Ethibond suture was used and knots were tied on top of duoderm for protection of the skin. The Velcro hook portion was affixed to the right abdomen in the same fashion. The Wittmann patch was approximated to the size of the wound, measuring 25 centimeters long by 15 centimeters wide. The abdomen was pushed closed while monitoring bladder pressures the entire time. The fascial distance ultimately measured 7 centimeters in diameter. On post-operative day 8 of Wittmann patch placement, abdominal closure was successfully achieved.
Discussion: We present our case where the impact of the Wittmann Patch was proven successful to close the abdomen, without requiring a mesh. The Wittmann Patch approach has kept our patient clinically stable.