Abstract
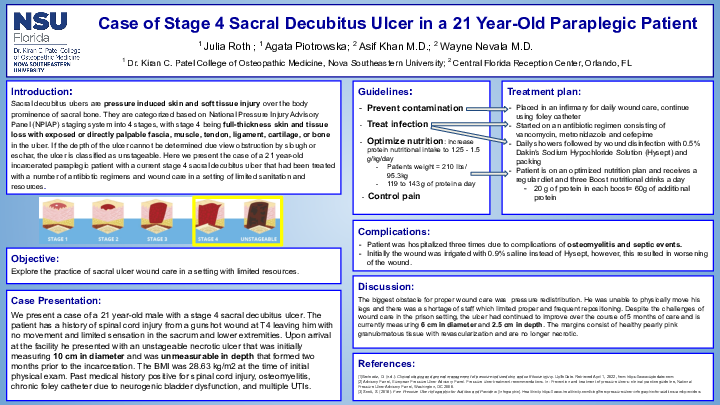
Introduction: Sacral decubitus ulcers are pressure-induced skin and soft tissue injuries over the body prominence of the sacral bone. They are categorized based on National Pressure Injury Advisory Panel (NPIAP) staging system into 4 stages, with stage 4 being full-thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage, or bone in the ulcer. If the depth of the ulcer cannot be determined due to obstruction by slough or eschar, the ulcer is classified as unstageable. Here we present the case of a 21-year-old incarcerated paraplegic patient with a current stage 4 sacral decubitus ulcer that had been treated with several antibiotic regimens and wound care in a setting of limited sanitation and resources.
Case Description: We present a case of a 21-year-old male with a stage 4 sacral decubitus ulcer. The patient has a history of spinal cord injury from a gunshot wound at T4 leaving him with no movement and limited sensation in the sacrum and lower extremities. Upon arrival at the facility, he presented with an unstageable necrotic ulcer that was initially measuring 10 cm in diameter and was unmeasurable in depth that formed two months before his incarceration. His BMI was 28.63 kg/m2 at the time of the initial physical exam. Past medical history is positive for spinal cord injury, osteomyelitis, chronic foley catheter due to neurogenic bladder dysfunction, and multiple UTIs. He was placed in an infirmary for wound daily wound care and started on an antibiotic regimen consisting of vancomycin, metronidazole, and cefepime. The patient was hospitalized three times due to complications of osteomyelitis and septic events. The current wound care plan includes daily showers followed by wound disinfection with 0.5% Dakin’s Sodium Hypochloride Solution (Hysept) and packing. Initially, the wound was irrigated with 0.9% saline instead of Hysept, however, this resulted in the worsening of the wound. The patient is on an optimized nutrition plan and receives 3 Ensure Boots a day in addition to a regular diet. Despite the challenges of wound care in the prison setting, the ulcer continued to improve over 5 months of care and is currently measuring 6 cm in diameter and 2.5 cm in depth. The margins consist of healthy pearly pink granulomatous tissue with revascularization and are no longer necrotic.
Discussion: A sacral decubitus ulcer is a common injury in paraplegic patients due to a lack of sensation and movement. The treatment plan includes infection control, optimization of nutrition, redistribution of pressure, and contamination prevention. This case aims to demonstrate the challenges of wound care in a setting of limited resources and poor sanitation as well as the need for creative medical approaches for the best patient outcomes.