Abstract
Introduction: Chronic headaches and neck pain are both challenging conditions to manage that can severely impact a patient’s quality of life. Treatment options vary widely and can lead to variable responses to therapy, both positive and negative. This case highlights a male patient suffering from more than a decade of debilitating headaches and neck pain who presented to the osteopathic manipulative medicine (OMM) clinic. Following the first visit the patient had an extremely favorable response to OMM leading to significantly reduced severity and frequency of both his headaches and neck pain.
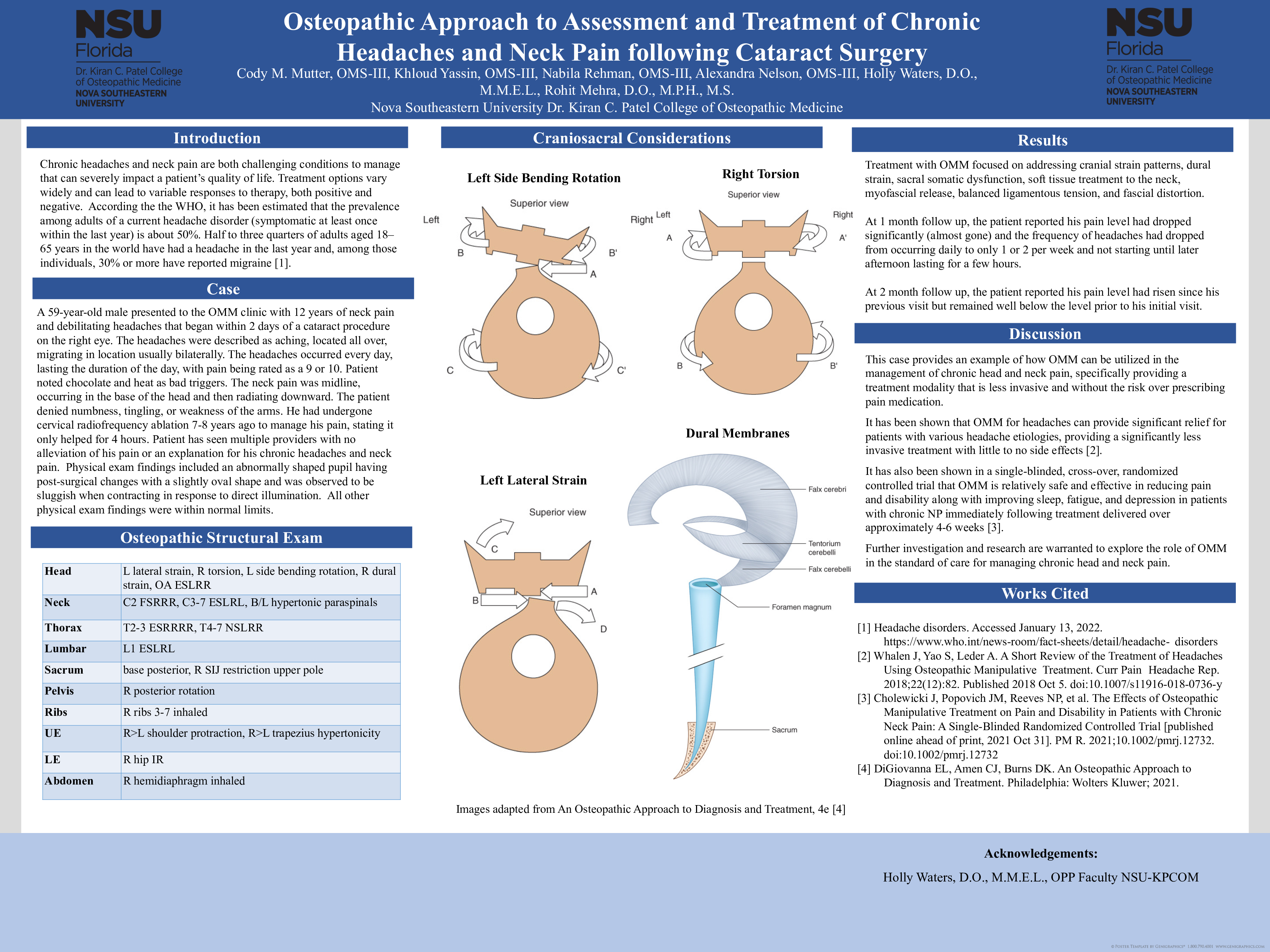
Case: A 59-year-old male presented to the OMM clinic with 12 years of neck pain and debilitating headaches that began within 2 days of a cataract procedure on the right eye. The headaches were described as aching, located all over, migrating in location usually bilaterally. The headaches occurred every day, lasting the duration of the day, with pain being rated as a 9 or 10. Patient noted chocolate and heat as bad triggers. The neck pain was midline, occurring in the base of the head and then radiating downward. The patient denied numbness, tingling, or weakness of the arms. He had undergone cervical radiofrequency ablation 7-8 years ago to manage his pain, stating it only helped for 4 hours. Patient has seen multiple providers with no alleviation of his pain or an explanation for his chronic headaches and neck pain. Physical exam findings included an abnormally shaped pupil having post-surgical changes with a slightly oval shape and was observed to be sluggish when contracting in response to direct illumination. All other physical exam findings were normal. Relevant osteopathic structural exam findings included specific findings for the head (left lateral strain, R torsion, L side bending rotation, R dural strain, OA ESLRR), neck (C2 FSRRR, C3-7 ESLRL, bilateral hypertonic paraspinals), sacrum (base posterior, R sacroiliac joint restriction upper pole), pelvis (R posterior rotation), upper extremity (R>L shoulder protracted, R>L trapezius hypertonicity), and abdomen (R hemidiaphragm inhaled).
Treatment with OMM focused on addressing cranial strain patterns, dural strain, sacral somatic dysfunction, soft tissue treatment to the neck, myofascial release, balanced ligamentous tension, and fascial distortion. At 1 month follow up, the patient reported his pain level had dropped significantly (almost gone) and the frequency of headaches had dropped from occurring daily to only 1 or 2 per week and not starting until later afternoon lasting for a few hours.
Discussion: This case provides an example of how OMM can be utilized in the management of chronic head and neck pain, specifically providing a treatment modality that is less invasive and without the risk over prescribing pain medication. Further investigation and research are warranted to explore the role of OMM in the standard of care for managing chronic head and neck pain.