Abstract
Introduction: Uterine leiomyomas, also referred to as fibroids, are the most common gynecological tumors in women. Symptoms include abnormal uterine bleeding, pelvic pain, and/or reproductive dysfunction. Giant leiomyomas are classified as those weighing more than 25lb (11.4 kg). They are exceedingly rare, with one literature review noting only 60 case reports worldwide in the last 50 years. Most patients with giant leiomyomas require surgical intervention, typically a hysterectomy that can obviate future fertility. Due to their extreme size, they significantly affect quality of life and impose a health risk that precludes medical management and warrant surgical intervention. Here, we present a case of a patient with a giant, 40-pound uterine leiomyoma that was successfully removed by myomectomy.
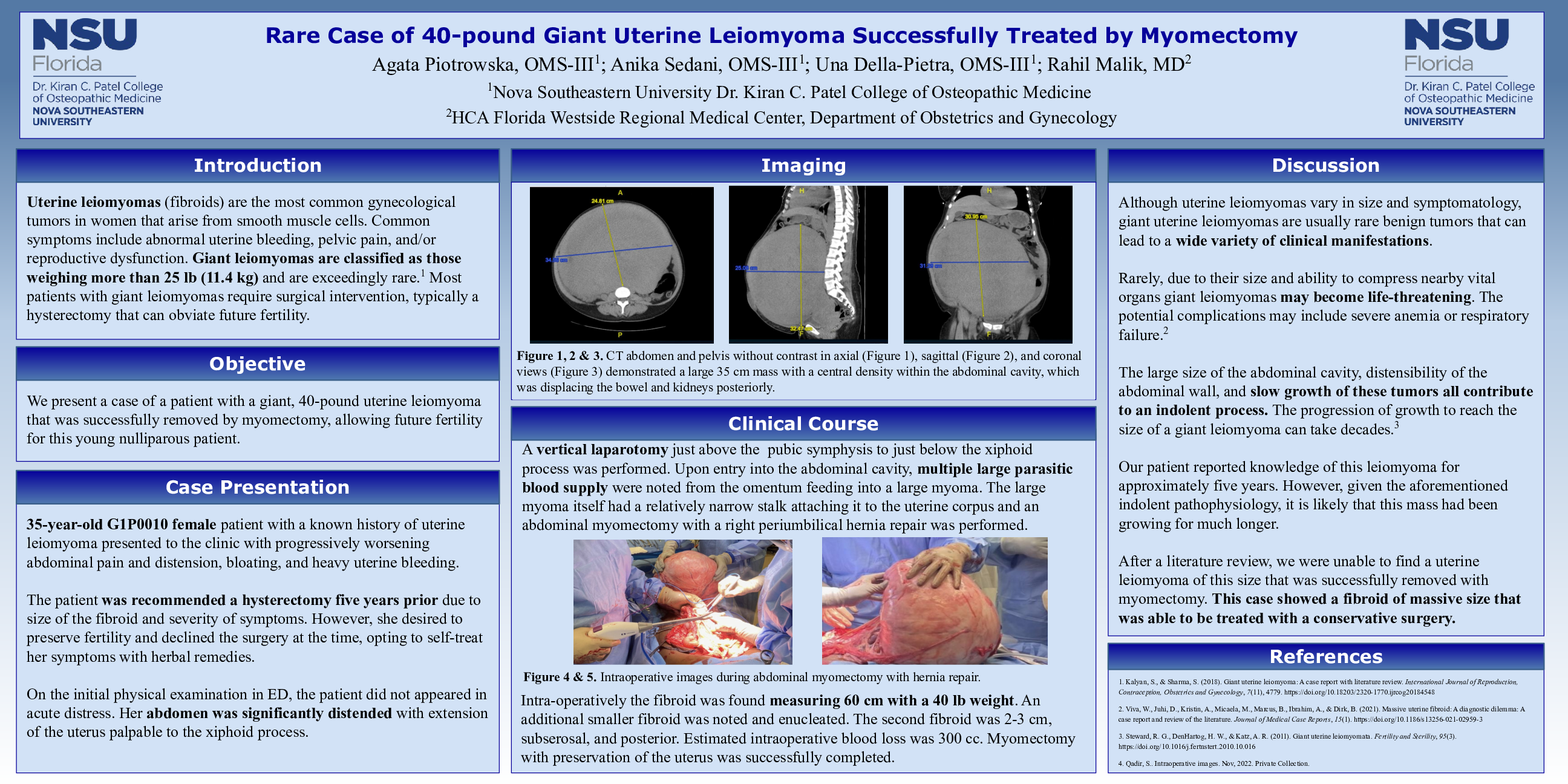
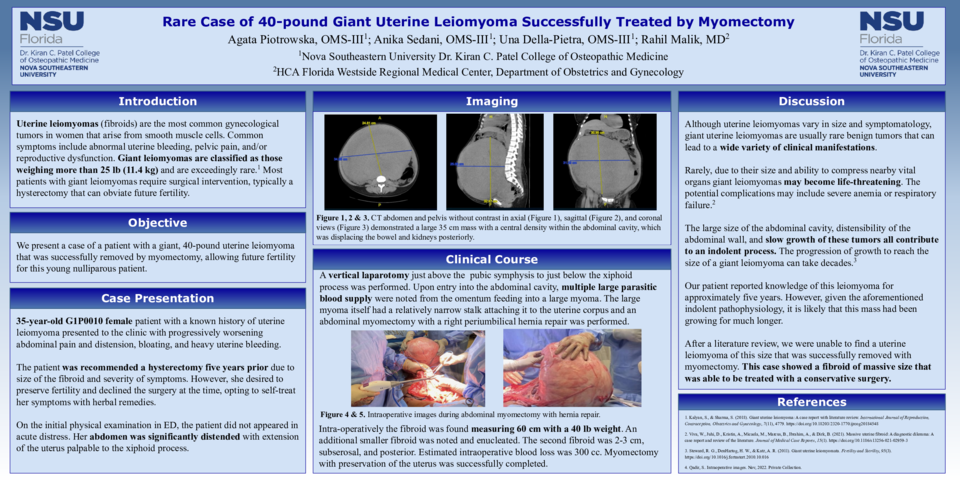
Case Description: A 35-year-old G1P0010 female patient with a known history of uterine leiomyoma presented to the clinic with progressively worsening abdominal pain and distension, bloating, and heavy uterine bleeding. The patient was seen by a gynecologist five years prior and was recommended a hysterectomy due to size of the fibroid and severity of symptoms. However, she declined at the time, opting to treat her fibroids with herbal remedies instead. Since the last gynecological evaluation, the symptoms had worsened, which prompted her to visit the emergency department. On the initial physical examination, the patient appeared in no acute distress. Her abdomen was significantly distended with extension of the uterus palpable at the xiphoid process. Right periumbilical hernia was noted. BMI was 33.7. CT abdomen and pelvis without contrast demonstrated a large 35 cm mass with a central density within the abdominal cavity, which was displacing the bowel and kidneys posteriorly. Gynecology was consulted. Patient denied inpatient surgery and opted for the outpatient evaluation with interval treatment for iron deficiency anemia due to menorrhagia. After review of CT scan and patient’s desire for future fertility, a myomectomy with possible hysterectomy was scheduled. A vertical laparotomy just above the pubic symphysis to just below the xiphoid process was performed. Upon entry into the abdominal cavity, large parasitic blood supply was noted from the omentum feeding into a large myoma. The myoma had a relatively narrow stalk attaching it to the uterine corpus and an abdominal myomectomy with a right periumbilical hernia repair was performed. Intra- operatively the fibroid was found to measure 60 cm and weight 40 lb. An additional 2-3 cm, sub- serosal, posterior fibroid was noted and enucleated. Estimated intraoperative blood loss was 300cc. Myomectomy with preservation of the uterus was successfully completed.
Discussion: Although uterine leiomyomas vary in size and symptomatology, giant uterine leiomyomas are usually rare benign tumors that can lead to a wide variety of clinical manifestations. The large size of the abdominal cavity, distensibility of the abdominal wall, and slow growth of these tumors all contribute to an indolent process. After a literature review, we were unable to find a uterine leiomyoma of this size that was successfully removed with myomectomy. This case showed a giant fibroid that was able to be treated with a conservative surgery.