Abstract
Background: Malignant psoas syndrome (MPS) is a rare clinical syndrome which significantly impacts the quality of life of cancer patients through its metastatic infiltration of the iliopsoas muscle. MPS is identified as a characteristic ipsilateral posture of fixed hip joint flexion associated with debilitating pain and poor prognosis for survival. The current literature describing the diagnostic criteria, management, and prognosis of MPS is limited primarily to case reports and literature reviews. There remains a gap in the current knowledge of MPS and in the management of this complex cancer-related pain syndrome. Thus, a scoping review was necessary to synthesize the available clinical evidence from case reports and case series.
Objective: This scoping review aimed to map current case reports and case series on MPS for diagnostic criteria, treatment modalities, and resulting prognoses of MPS in terminal cancer patients.
Method: A systematic search using the databases EMBASE and PubMed was conducted to access case reports and case series published between January 1990 and October 2022 that met the study’s inclusion criteria: 1) adult patients with metastatic cancer; 2) MPS symptoms secondary to infiltration of iliopsoas; 3) diagnostic criteria, treatment modality and prognosis; and 4) English-language text. Our search strategy yielded 1926 citations. After removing 629 duplicates, 1,282 reports were excluded due to failure to meet eligibility criteria (n=1,270) or inaccessibility (n=12). Using the JBI appraisal tools for case reports and case series, a total of 15 articles remained for inclusion in the scoping review. Four independent reviewers extracted and synthesized the data into tabular form and utilized an analytical approach to present the data.
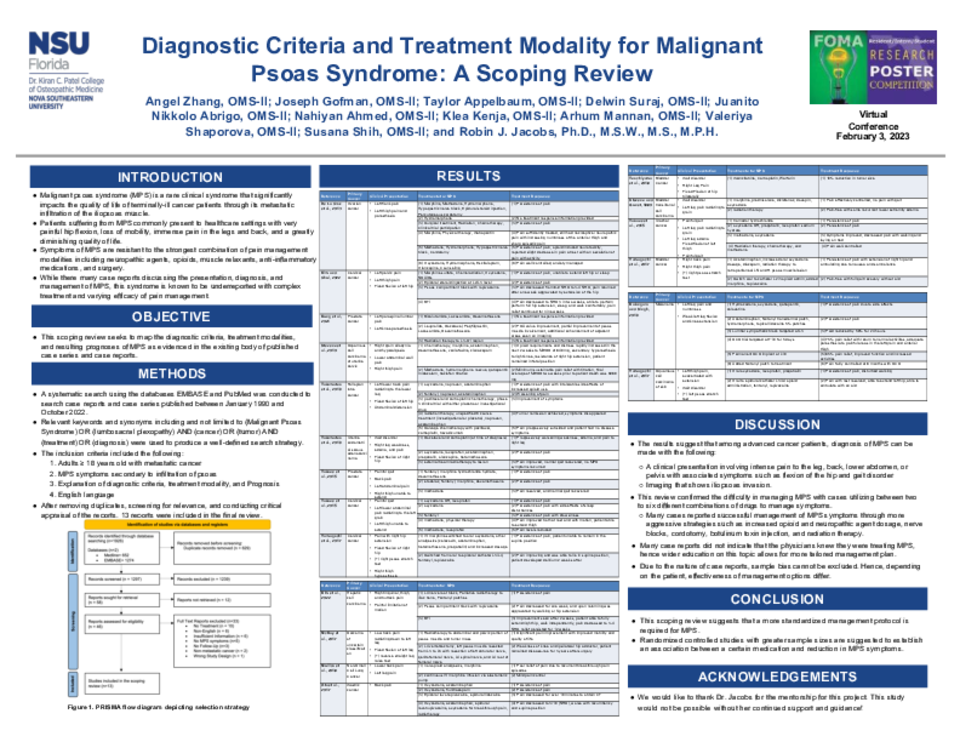
Results: Among the 15 included articles, the most common causative primary cancer was genital urinary cancer. Many cases reported first addressing the pain, using opioids for palliative care. Following a necessitated increase in morphine equivalent daily dose, a subsequent increase in strength of analgesic, change in route of administration such as epidural catheters, and integration of combination drug therapy provided overall improved symptom relief. As efficacy of analgesics decreased, palliative procedures such as radiation therapy, cordotomy, and nerve blocks were used, with various degrees of effectiveness. Patients died from their cancers either weeks or months after the first MPS diagnosis.
Conclusion: A unified clinical definition of MPS may be required to inform physicians of this syndrome to help make better clinical decisions regarding treatments for patients. The studies indicated that a clearer guideline for treatment protocol may be warranted as most cases show various treatment medication dosages and procedures with differing results. As MPS leads to both nociceptive and neuropathic pain, it may be indicated that treatments should respond to both types of pain to improve the quality of life in patients with MPS.