Abstract
Introduction: Subclavian steal syndrome (SSS) is a well-documented phenomenon resulting from a reversal of blood flow through the ipsilateral vertebral artery due to occlusion or stenosis of the subclavian artery proximal to the origin of the vertebral artery. This leads to a decrease in the normal anterograde flow of blood into the vertebral artery and theoretically, a decrease in the perfusion of the cerebral circulation. By and large, patients with subclavian steal syndrome are usually asymptomatic. However, when symptomatic, patients typically present with claudication, exercise intolerance of the upper extremities, or symptoms of vertebrobasilar insufficiency (VBI) such as vertigo and nystagmus. Here we report a case in which a patient presenting with complaints of right-handed “clumsiness,” mild generalized weakness, dizziness, and a few episodes of near syncope for a few weeks was found to have Subclavian Steal Syndrome due to hemodynamically significant stenosis of the innominate artery.
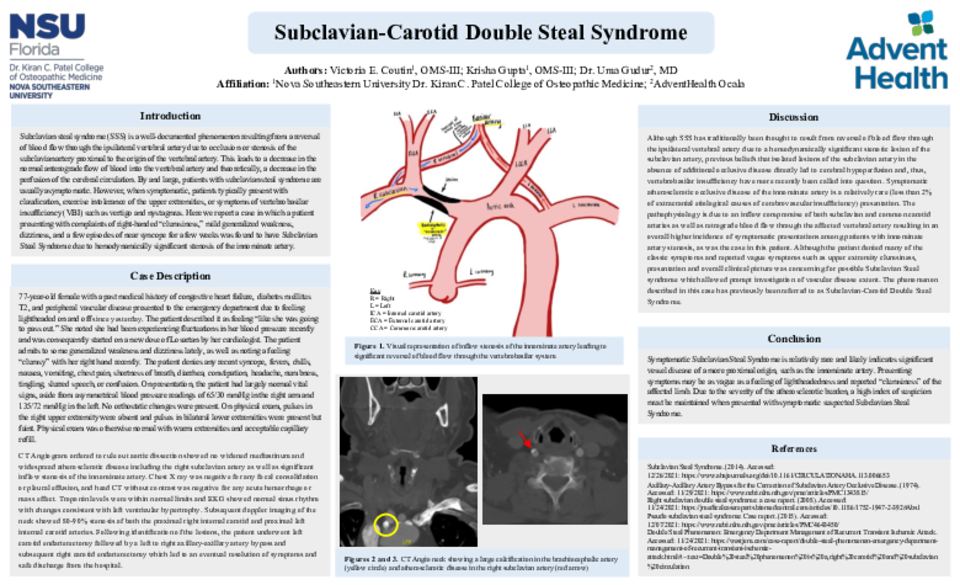
Case description: A 77-year-old female presented with episodes of feeling lightheaded and recent right-handed “clumsiness.” On presentation, the patient had asymmetrical blood pressure readings of 65/30 mmHg in the right arm and 135/72 mmHg in the left arm. Physical exam was positive for absent pulses in the right upper extremity and present, but faint pulses in bilateral lower extremities. Life-threatening cardiac, pulmonary, and neurologic etiologies such as aortic dissection and cerebrovascular accident were promptly investigated and ruled out. Presenting symptoms and overall clinical picture was concerning for possible subclavian steal syndrome. CT angiogram demonstrated diffuse atherosclerotic disease including the subclavian artery and significant inflow stenosis of the right innominate artery. Subsequent doppler imaging of the neck revealed atherosclerotic disease of both carotid arteries and retrograde flow down the right vertebral artery. Throughout the course of the hospital stay, the patient underwent a left carotid endarterectomy followed by a left to right axillary-axillary artery bypass and a subsequent right carotid endarterectomy leading to an eventual resolution of symptoms and safe discharge from the hospital.
Discussion: Although SSS has traditionally been thought to result from reversal of blood flow through the ipsilateral vertebral artery due to a hemodynamically significant lesion of the subclavian artery, previous beliefs that lesions of the subclavian artery in the absence of additional occlusive disease directly lead to cerebral hypoperfusion and vertebrobasilar insufficiency have more recently been called into question. Symptomatic atherosclerotic occlusive disease of the innominate artery is a relatively rare presentation, accounting for less than 2% of extracranial etiological causes of cerebrovascular insufficiency. The pathophysiology is due to an inflow compromise of both subclavian and common carotid arteries, resulting in an overall higher incidence of symptomatic presentations among patients with innominate artery stenosis, as was the case in this patient.



