Abstract
Introduction
Neural tube defects (NTDs) are significant congenital anomalies of the central nervous system affecting every 1 in 1000 pregnancies. The causes include failure of neurulation happening around the 28th day after conception, non-compliance to folic acid supplements, and consumption of antiepileptic medication. Spina bifida is the most common congenital malformation of the spine, in which failure of fusion of posterior laminar vertebrae occurs with or without developmental defect of the spinal cord. Based on the presentation, such cases are classified as occulta (mild type) or cystica (severe form including meningocele and meningomyelocele).
Case description
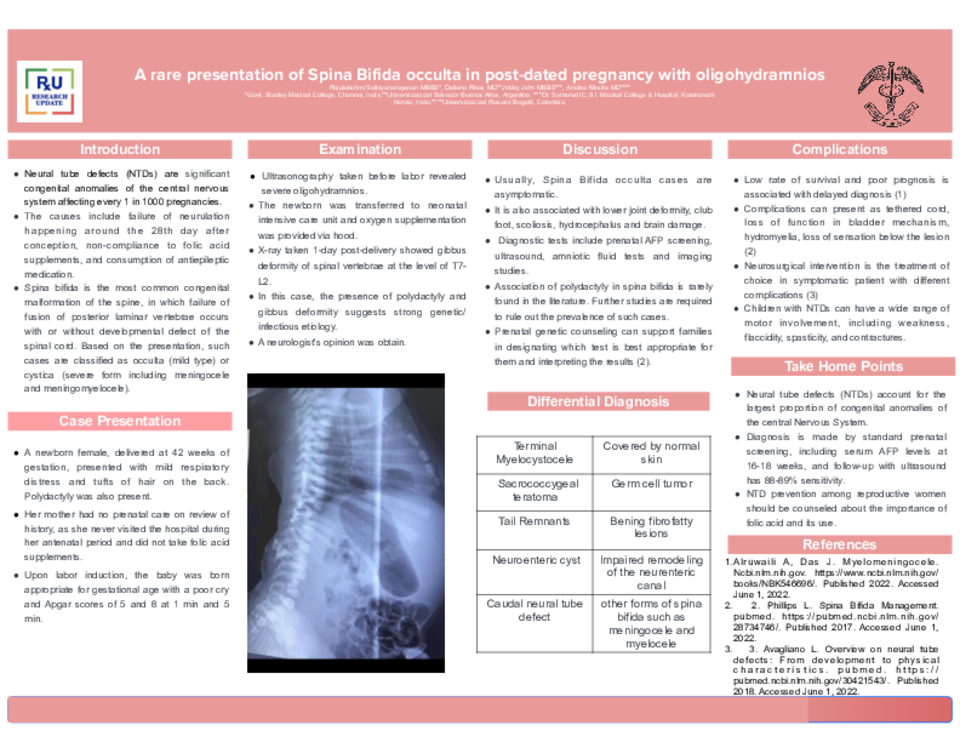
A newborn female, delivered at 42 weeks of gestation, presented with mild respiratory distress and tufts of hair on the back. Polydactyly was also present. Her mother had no prenatal care on review of history, as she never visited the hospital during her antenatal period and did not take folic acid supplements. Ultrasonography taken before labor revealed severe oligohydramnios, a common manifestation of post-dated pregnancy. Upon labor induction, the baby was born appropriate for gestational age with a poor cry and Apgar scores of 5 and 8 at 1 min and 5 min The newborn was transferred to neonatal intensive care unit and oxygen supplementation was provided via hood. X-ray taken 1-day post-delivery showed gibbus deformity of spinal vertebrae at the level of T7-L2. A neurologist's opinion was obtained.
Conclusion
Usually, Spina Bifida occulta cases are asymptomatic. It is also associated with lower joint deformity, club foot, scoliosis, hydrocephalus and brain damage. Diagnostic tests include prenatal AFP screening, ultrasound, amniotic fluid tests and imaging studies. In this case, the presence of polydactyly and gibbus deformity suggests strong genetic/infectious etiology. Association of polydactyly in spina bifida is rarely found in the literature. Further studies are required to rule out the prevalence of such cases.
Neural tube defects (NTDs) account for the largest proportion of congenital anomalies of the central Nervous System and result from failure of the neural tube to close. Diagnosis is made by standard prenatal screening, including serum AFP levels at 16-18 weeks, and follow-up with ultrasound has 88-89% sensitivity. Children with NTDs can have a wide range of motor involvement, including weakness, flaccidity, spasticity, and contractures. NTD prevention among reproductive women should be counseled about the importance of folic acid and its use. Treatment includes surgical correction and cooperation by multidisciplinary specialists.



