Abstract
Introduction: Kartagener Syndrome (KS) is an autosomal recessive disorder classified as a subtype of Primary Ciliary Dyskinesia (PCD) that involves situs inversus, bronchiectasis, and recurrent sinusitis. The predominant defect that characterizes PCD is mutated dynein, leading to dysfunctional microtubules [1]. Clinical features include, but are not limited to, recurrent ear and sinus infections and infertility due to insufficient sperm motility. Mutations in genes such as dynein axonemal heavy chain 11 (DNAH11) and dyslexia susceptibility 1 candidate 1 gene (DYX1c1) have been associated with dysfunctional cilia and contribute to PCD. These genes have also been studied for their role in dyslexia and other neurodevelopmental conditions, (i.e. Autism Spectrum Disorder (ASD)) [2]. In one specific study, there was a higher prevalence of neurodevelopmental issues (i.e. communication delays) in elementary school children with PCD when compared to age-matched controls and subjects with cystic fibrosis [3]. Other studies have reported left-right axis abnormalities in the brain associated with ciliopathies, indicating possible association with neurodevelopmental disorders [4].
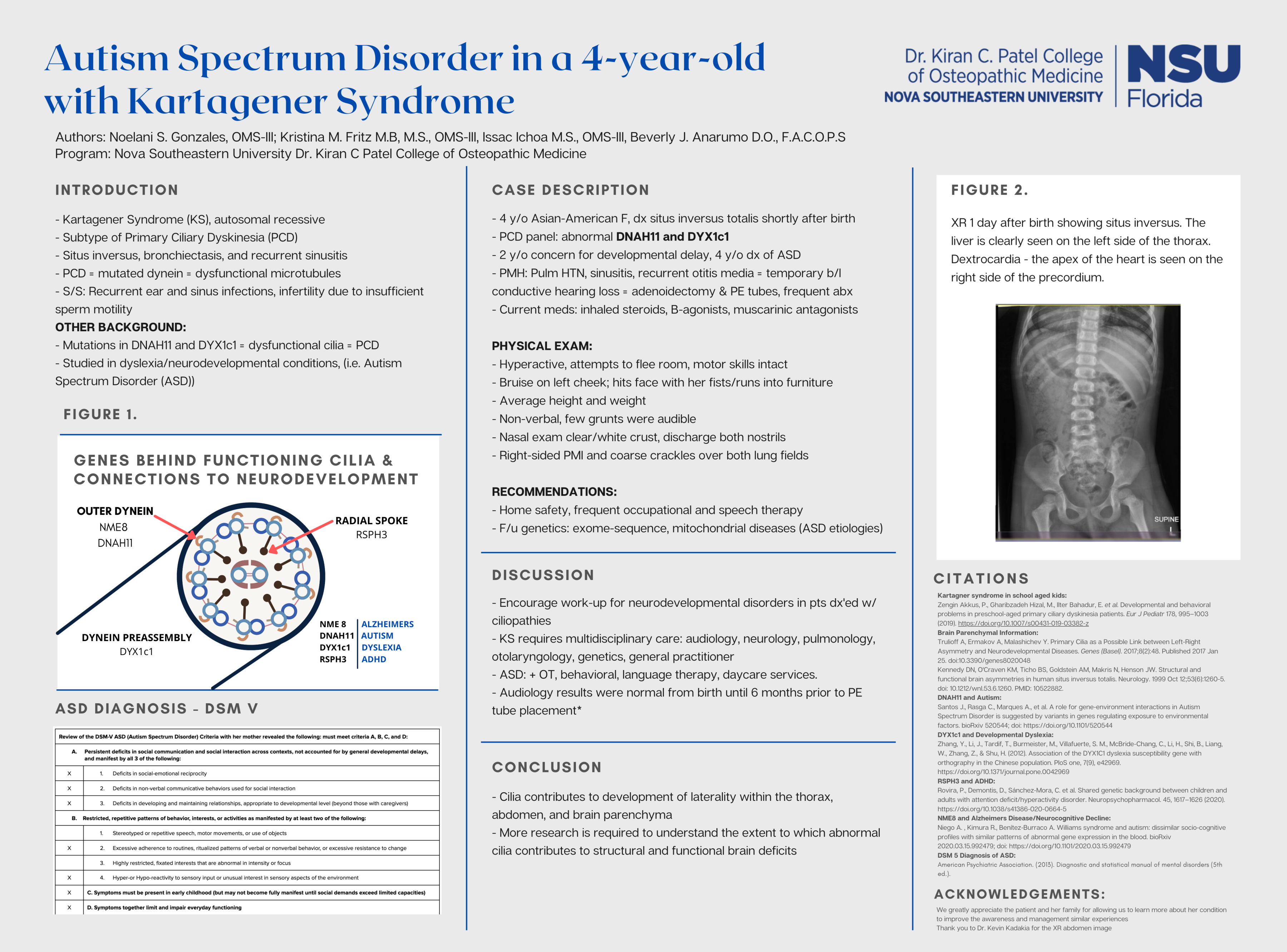
Case Description: Discussed in this case report is a 4-year-old Asian-American female diagnosed with situs inversus totalis shortly after birth. A PCD panel resulted in abnormal variants in genes including DNAH11 and DYX1c1. Around 2-years-old, there was concern for developmental delay. At 4-years-old, she was formally diagnosed with ASD. The etiology of her ASD remains unclear. Her past medical history includes pulmonary hypertension, maxillary sinusitis, recurrent otitis media leading to temporary bilateral conductive hearing loss necessitating adenoidectomy and pressure equalizing tube placement. Repeated infections required frequent use of antibiotics. Current long-term medications include inhaled steroids, beta-agonists, and muscarinic antagonists. The patient presented as a hyperactive female of average height and weight. She was non-verbal, but a few grunts were audible. The patient had a bruise on her left cheek; reportedly from hitting her face with her fists or running into furniture at home. She regularly attempted to flee the room, and after one successful escape, put her hands into the toilet. Her motor skills appeared fully intact. Auscultation of the precordium revealed right-sided PMI and coarse crackles over both lung fields. Her ears were unable to be examined due to her inability to keep still, even when restrained by her mother. Nasal examination showed clear/white crust and discharge from both nostrils. Increased home safety measures and frequency of occupational therapy (OT) and speech therapy were recommended to improve communication and behavior. Follow up with her geneticist to obtain exome-sequencing and mitochondrial disease screening was advised to help determine etiology of ASD.
Discussion: A goal of this case report is to encourage work-up for neurodevelopmental disorders in patients diagnosed with ciliopathies. KS requires multidisciplinary care entailing frequent exams with audiology, neurology, pulmonology, otolaryngology, genetics, and a general practitioner. ASD adds another dimension to this patient’s care, requiring OT, behavioral, and language therapy, and specialized daycare services.