Abstract
Background:
Dengue and Chikungunya co-infection is characterized by fever and severe arthralgia. The Aedes mosquitoes are the common vectors for both. Its manifestation as vesiculobullous lesions is both rare and interesting, as the bullous rash can be easily mistaken as an autoimmune disease.
Case Presentation:
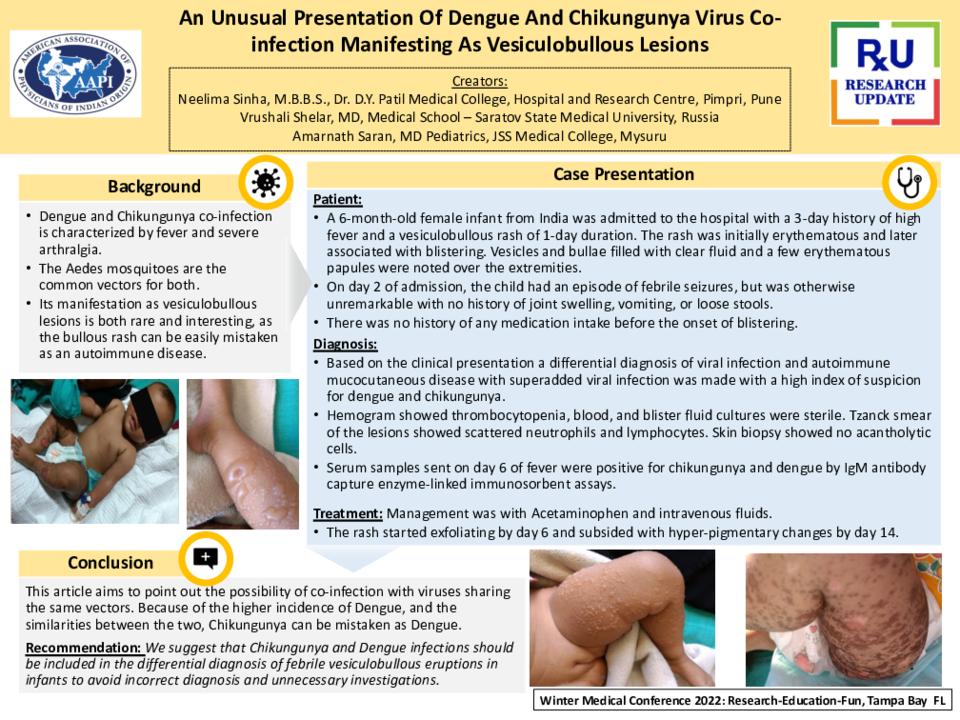
A 6-month-old female infant from India was admitted to the hospital with a 3-day history of high fever and a vesiculobullous rash of 1-day duration. The rash was initially erythematous and later associated with blistering. Vesicles and bullae filled with clear fluid and a few erythematous papules were noted over the extremities. On day 2 of admission, the child had an episode of febrile seizures, but was otherwise unremarkable with no history of joint swelling, vomiting, or loose stools. There was no history of any medication intake before the onset of blistering. Based on the clinical presentation a differential diagnosis of viral infection and autoimmune mucocutaneous disease with superadded viral infection was made with a high index of suspicion for dengue and chikungunya. Hemogram showed thrombocytopenia, blood, and blister fluid cultures were sterile. Tzanck smear of the lesions showed scattered neutrophils and lymphocytes. Skin biopsy showed no acantholytic cells. Serum samples sent on day 6 of fever were positive for chikungunya and dengue by IgM antibody capture enzyme-linked immunosorbent assays. Management was with Acetaminophen and intravenous fluids. The rash started exfoliating by day 6 and subsided with hyperpigmentary changes by day 14.
Conclusion:
This article aims to point out the possibility of co-infection with viruses sharing the same vectors. Because of the higher incidence of Dengue, and the similarities between the two, Chikungunya can be mistaken as Dengue. We suggest that Chikungunya and Dengue infections should be included in the differential diagnosis of febrile vesiculobullous eruptions in infants to avoid incorrect diagnosis and unnecessary investigations.