Abstract
Introduction: Gastric mesenchymal neoplasms are rare tumors that develop as well-circumscribed intramural or submucosal masses. Most commonly (up to 90%), mesenchymal tumors of the stomach originate from the interstitial cells of Cajal and are known as gastrointestinal stromal tumors (GISTs). Rarely, gastric schwannomas (GS) develop from the Schwann cells in Auerbach’s myenteric plexus. GS account for only 0.2% of all gastric tumors. It is crucial to differentiate between these two neoplasms since their prognosis differs significantly. GISTs have rapid growth and potential malignant transformation, whereas GS are slow-growing benign tumors. Most reported cases of GS are after the sixth decade of life. Therefore, it is essential to consider this often-overlooked diagnosis in the differential of submucosal gastric masses in a rapidly aging population.
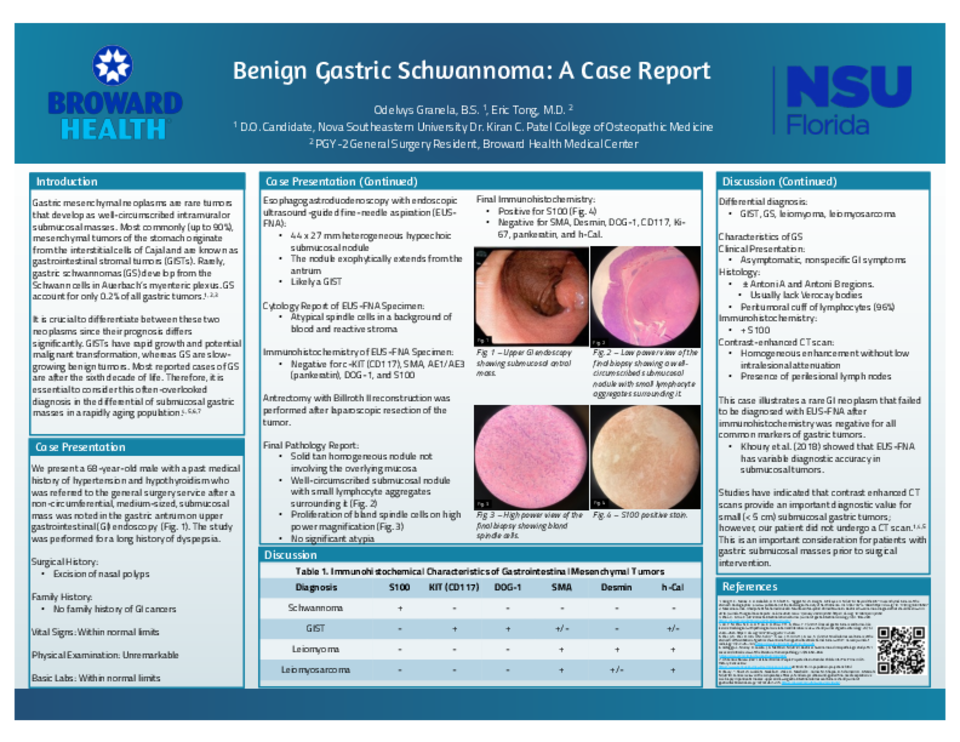
Case Description: We present a 68-year-old male with a past medical history of hypertension and hypothyroidism who was referred to the general surgery service after a non-circumferential, medium-sized, submucosal mass was noted in the gastric antrum on upper gastrointestinal (GI) endoscopy. The study was performed for a long history of dyspepsia. Past surgical history was remarkable for excision of nasal polyps. The patient had no family history of GI cancers. Vital signs, physical examination, and basic laboratory studies were within normal limits. Esophagogastroduodenoscopy with endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) showed a 4.4 x 2.7 cm heterogeneous hypoechoic submucosal nodule exophytically extending from the antrum and was characterized as likely a GIST. The pathology report indicated atypical spindle cells in a background of blood and reactive stroma. Immunohistochemistry of the biopsied tissue was negative for c-KIT, SMA, AE1/AE3, discovered on GIST-1 (DOG-1), and S100. The patient underwent laparoscopic surgery. The GI India ink tattoo was away from the mass, which increased intraoperative challenge and antrectomy with Billroth II reconstruction was performed. The resected mass was 3.5 x 3.5 cm. Final histopathology report showed bland proliferation of spindle cells containing Antoni A and Antoni B regions and a peritumoral cuff of lymphocytes. Immunohistochemical stains were positive for S100 and negative for CD117, DOG-1, Ki-67, Desmin, SMA, pankeratin, and Caldesmon. The patient had a prolonged hospital course secondary to postoperative complications including duodenal stump leak, pneumonia, and arrhythmia. He was discharged on postoperative day 24 with a duodenal stump drain in place.
Discussion: This case illustrates a rare GI neoplasm that failed to be diagnosed with EUS-FNA after immunohistochemistry was negative for all common markers of gastric tumors. After tumor resection, histologic findings and immunohistochemical evaluation positive for S100 confirmed the diagnosis of benign GS. Some studies have shown that EUS-FNA has variable diagnostic accuracy in submucosal tumors. Other studies have indicated that CT scans can provide good diagnostic value for small (< 5.0 cm) submucosal gastric tumors but is not currently considered the main diagnostic modality and our patient did not undergo a CT scan. This is an important consideration for patients with small gastric submucosal masses prior to surgical intervention.