Abstract
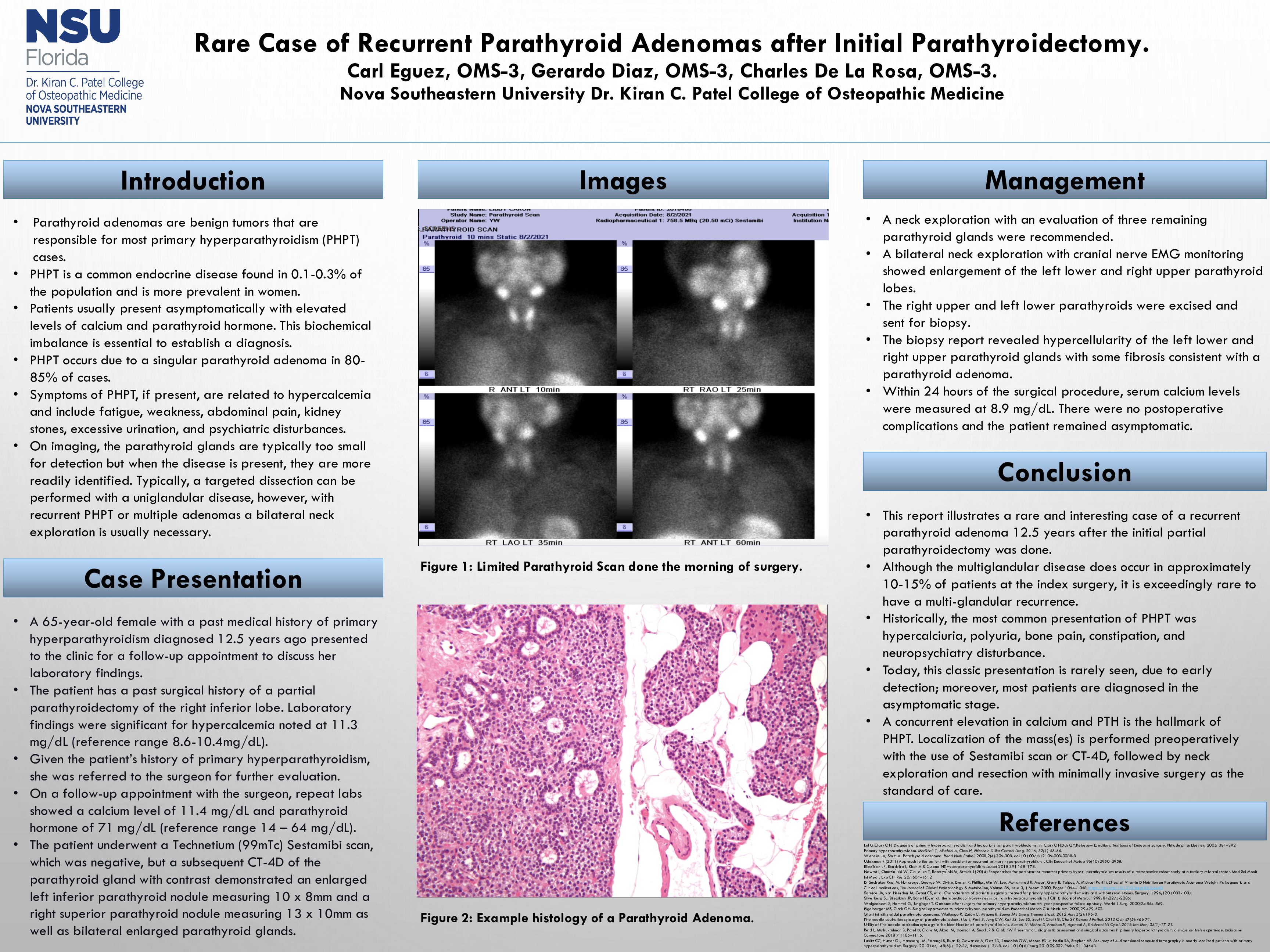
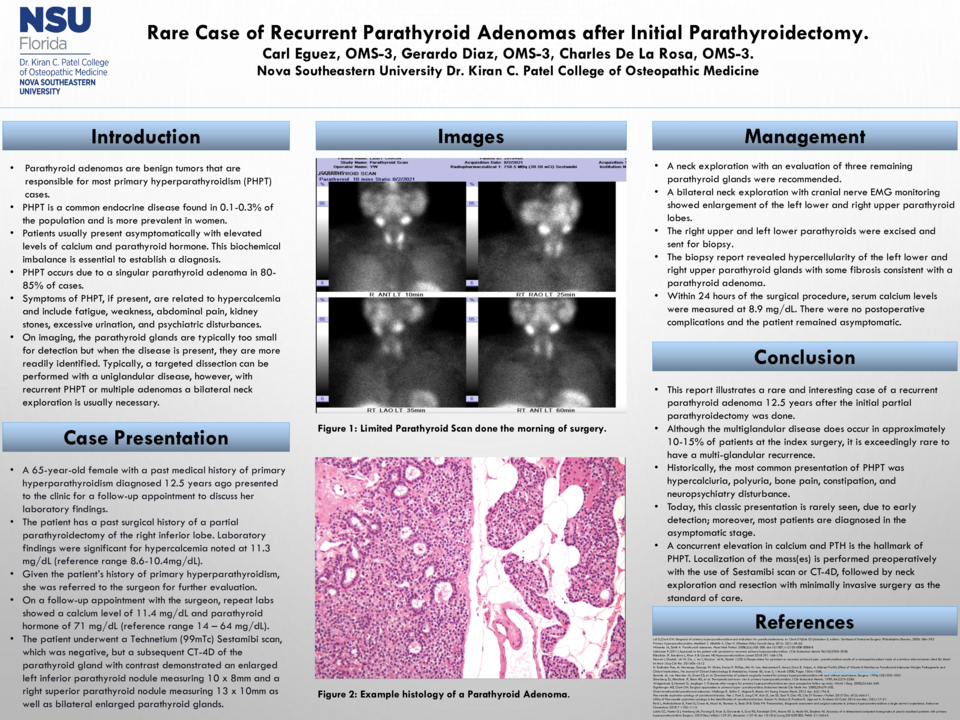
Case Description: We present a case of a 65-year-old female with a past medical history of primary hyperparathyroidism who presented to the clinic for a follow-up appointment to discuss her laboratory findings. During the visit, she stated that she is asymptomatic and denies any depression, constipation, dysuria, hematuria, or any cognitive changes. She has a past medical history of primary hyperparathyroidism diagnosed 12.5 years ago. She also has a history of anxiety, gastritis, hypercholesteremia, and gastroesophageal reflux disease. The patient has a past surgical history of a partial parathyroidectomy of the right inferior lobe. She is currently taking cholecalciferol and omeprazole. Laboratory findings were significant for hypercalcemia noted at 11.3 mg/dL (reference range 8.6-10.4mg/dL). Given the patient’s history of primary hyperparathyroidism, she was referred to the surgeon for further evaluation. On a follow-up appointment with the surgeon, repeat labs showed a calcium level of 11.4 mg/dL, ionized calcium of 6.3mg/dL (reference range 4.8 – 5.6mg/dL) and parathyroid hormone of 71 mg/dL (reference range 14 – 64 mg/dL). The patient underwent a Technetium (99mTc) Sestamibi scan, which was negative, but a subsequent CT-4D of the parathyroid gland with contrast demonstrated an enlarged left inferior parathyroid nodule measuring 10 x 8mm and a right superior parathyroid nodule measuring 13 x 10mm as well as bilateral enlarged parathyroid glands. A neck exploration with an evaluation of the three remaining parathyroid glands was recommended. A bilateral neck exploration with cranial nerve EMG monitoring showed enlargement of the left lower and right upper parathyroid lobes. The right upper and left lower parathyroids were excised and sent for biopsy. The biopsy report revealed hypercellularity of the left lower and right upper parathyroid glands with some fibrosis consistent with a parathyroid adenoma. Within 24 hours of the surgical procedure, serum calcium levels were measured at 8.9 mg/dL. There were no postoperative complications and the patient remained asymptomatic.
Discussion: This report illustrates a rare and interesting case of a recurrent parathyroid adenoma 12.5 years after the initial partial parathyroidectomy was done. Although the multiglandular disease does occur in approximately 10-15% of patients at the index surgery, it is exceedingly rare to have a multi-glandular recurrence. Historically, the most common presentation of PHPT was hypercalciuria, polyuria, bone pain, constipation, and neuropsychiatry disturbance. Today, this classic presentation is rarely seen, due to early detection; moreover, most patients are diagnosed in the asymptomatic stage. A concurrent elevation in calcium and PTH is the hallmark of PHPT. Localization of the mass(es) is performed preoperatively with the use of Sestamibi scan or CT-4D, followed by neck exploration and resection with minimally invasive surgery as the standard of care.