Abstract
Background: Femoral shaft fractures are one of the most common orthopedic fractures in the pediatric population, with fractures of the tibia being the third most common long bone fracture. Treatment of femoral and tibial fractures varies based on fracture morphology and age. This review will focus on operative modalities, including submuscular plating (SP) and flexible intramedullary nailing (FIN) for the treatment of femoral and tibial fractures in the pediatric population. Currently, the gold standard for treating length stable fractures in the femur and tibia of pediatric patients is FIN. However, children >11 years of age or >49kg in weight are at increased risk of complications. Therefore, postoperative immobilization with a single-leg walking spica cast, hip-knee-ankle-foot orthosis (HKAFO), or knee immobilizer can increase stability and reduce rates of complication. In contrast, submuscular plating (SP) is an equal, alternative operative modality that has not been well-established. Patients with SP require no postoperative mobilization and may be more beneficial in heavier patients.
Objective: The objective of this study is to perform a literature review comparing these two treatment modalities and to establish no difference in outcomes regarding time to healing, functional outcomes, quality of reduction, and time taken to remove hardware.
Methods: A literature search of PubMed articles published within the last 10 years was done. Inclusion criteria involved submuscular plating or flexible intramedullary nailing in femur or tibia fractures in those 1-17 years of age. Pathologic fractures, metabolic bone diseases, and neuromuscular disorders were excluded from the analysis. Time to healing, return to activity, overgrowth at fracture site, time after surgery to hardware removal, rate of nonunion, and rate of malunion were the outcomes of interest. A total of 25 publications met these criteria.
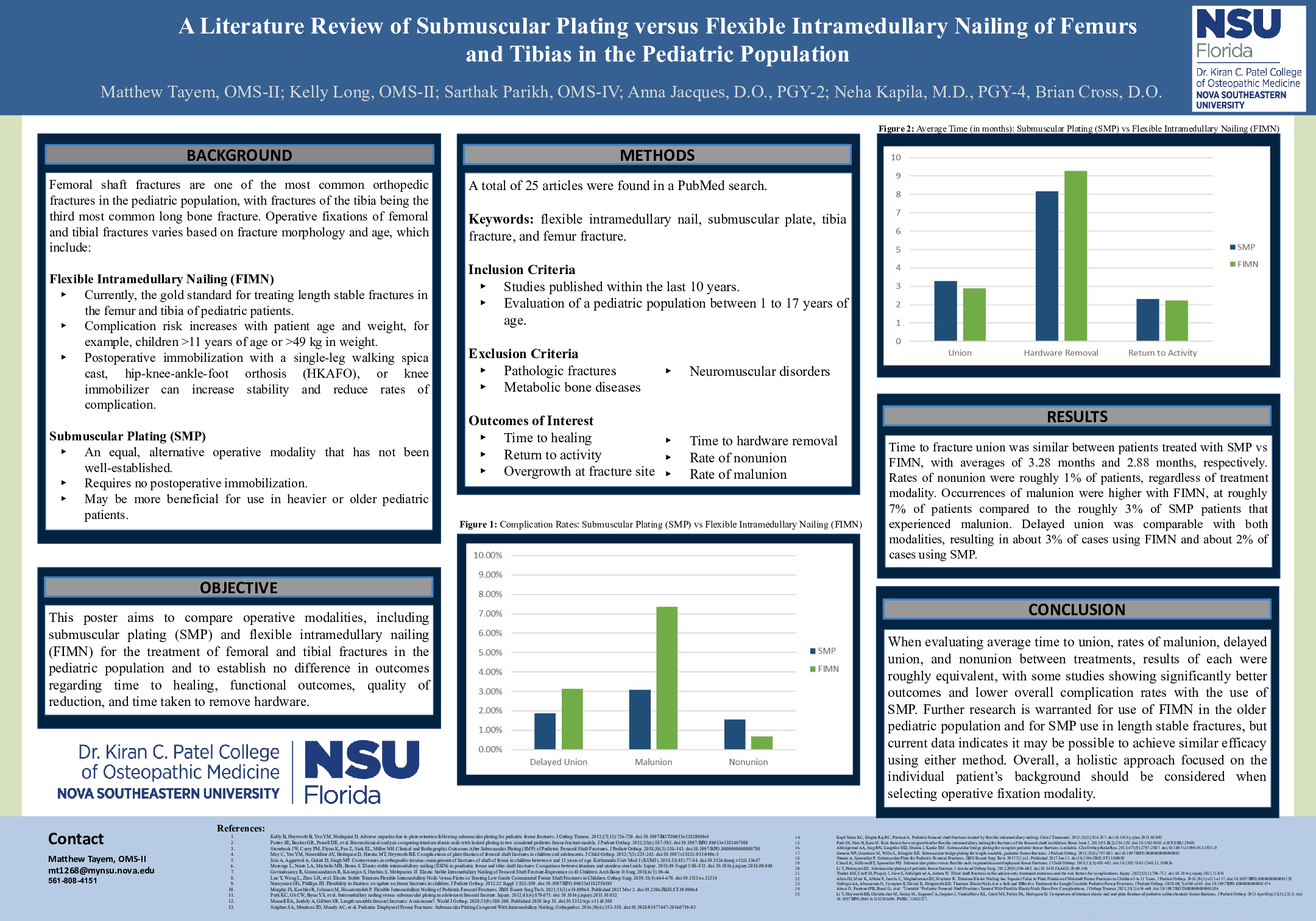
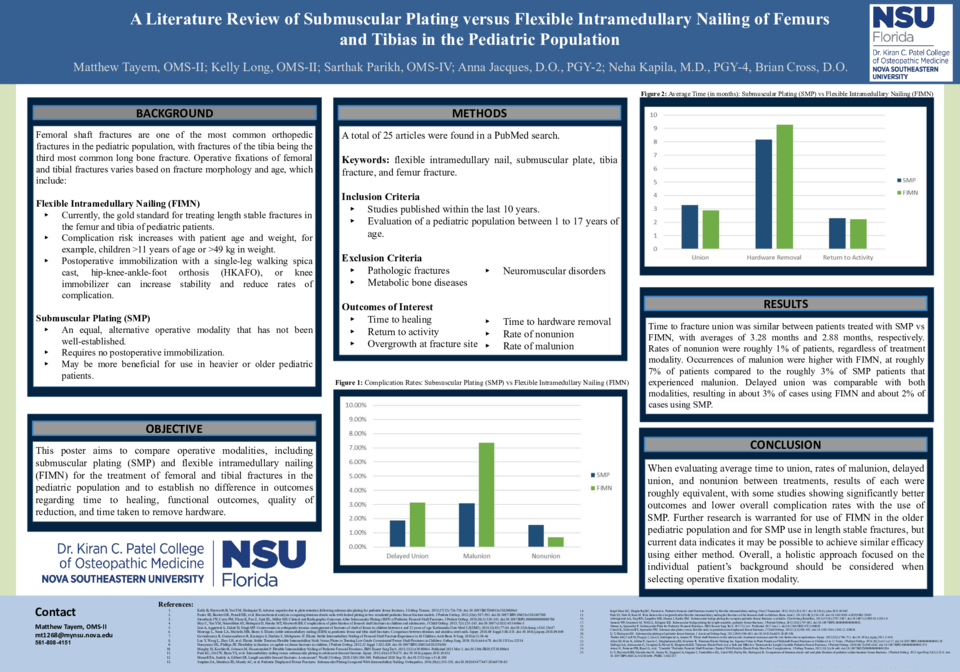
Results: Time to fracture union was similar between patients treated with submuscular plating vs flexible intramedullary nailing, with averages of 3.28 months and 2.88 months, respectively. Rates of nonunion were roughly 1% of patients, regardless of treatment modality. Occurrences of malunion were higher with flexible intramedullary nails, at roughly 7% of patients compared to the roughly 3% of submuscular plate patients that experienced malunion. Delayed union was comparable with both modalities, resulting in about 3% of cases using flexible intramedullary nails and about 2% of cases using submuscular plating.
Conclusion: When evaluating average time to union, rates of malunion, delayed union, and nonunion between both treatment modalities, results of each were roughly equivalent, with some studies showing significantly better outcomes and lower overall complication rates with the use of submuscular plating. Further research is warranted for use of flexible intramedullary nails in the older pediatric population and for submuscular plate use in length stable fractures, but current data indicates it may be possible to achieve similar efficacy using either method.