Abstract
Introduction: Colorectal carcinoma is the second most common cause of cancer-related deaths. About 25% of cecal adenocarcinomas present as acute appendicitis with 62% of them going undiagnosed as cancer. This delay in diagnosis can lead to poor outcomes and complications.
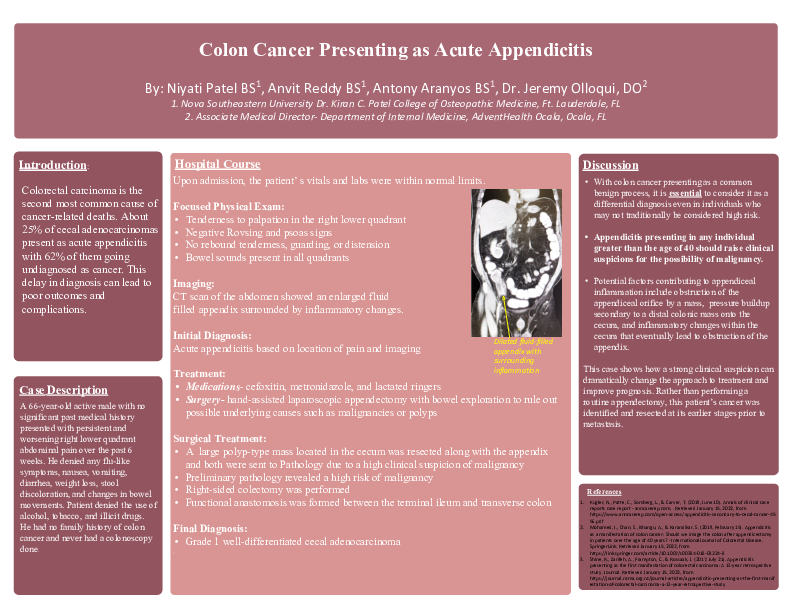
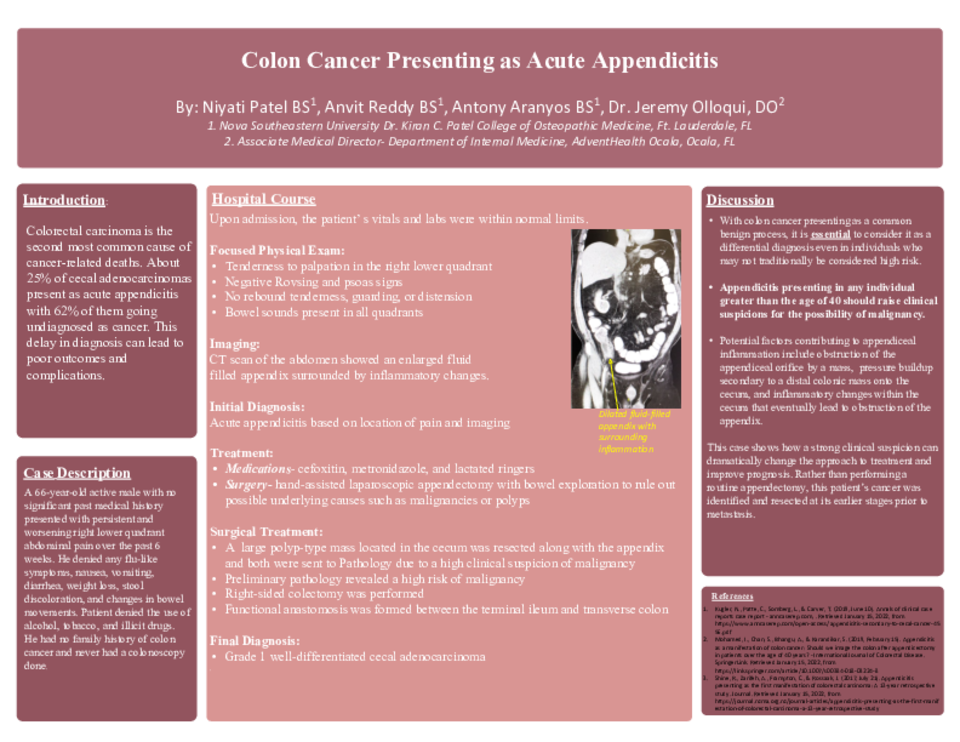
Case Description: A 66-year-old active male with no significant past medical history presented with persistent and worsening right lower quadrant abdominal pain lasting for 6 weeks. He denied any flu-like symptoms, nausea, vomiting, diarrhea, weight loss, stool discoloration, and changes in bowel movements. The patient denied the use of alcohol, tobacco, and illicit drugs. He had no family history of colon cancer and never had a colonoscopy done. Upon admission, the patient’s labs and vitals were within normal limits. On a focused physical exam, the patient had tenderness to palpation in the right lower quadrant and had negative Rovsing’s and psoas signs. There was no rebound tenderness, guarding, or abdominal distension. Bowel sounds were present in all quadrants. A CT scan of the abdomen showed an enlarged fluid-filled appendix surrounded by inflammatory changes. Based on the patient’s location of pain and imaging results, he was originally diagnosed with acute appendicitis. The patient was scheduled for a hand-assisted laparoscopic appendectomy with bowel exploration to rule out possible underlying causes such as malignancies or polyps. Medical management prior to surgery included cefoxitin, metronidazole, and lactated ringers. During surgery, a large polyp-type mass located in the cecum was resected along with the appendix and both were sent to Pathology due to a high clinical suspicion of malignancy. Preliminary pathology revealed a high risk of malignancy, so a right-sided colectomy was performed. As a result, a functional anastomosis was formed between the terminal ileum and transverse colon. Final pathology reports revealed a grade 1 well-differentiated cecal adenocarcinoma.
Conclusion/Discussion: With colon cancer presenting as a common benign process, it is essential to consider it as a differential diagnosis even in individuals who may not traditionally be considered high risk. Appendicitis presenting in any individual greater than the age of 40 should raise clinical suspicions for the possibility of malignancy. Therefore, any patient older than 40 who underwent a traditional appendectomy should be highly recommended to schedule a follow up colonoscopy 6 weeks after surgery. Potential factors contributing to appendiceal inflammation include obstruction of the appendiceal orifice by a mass, pressure buildup secondary to a distal colonic mass onto the cecum, and inflammatory changes within the cecum that eventually lead to obstruction of the appendix. This case shows how a strong clinical suspicion can dramatically change the approach to treatment and improve prognosis. Rather than performing a routine appendectomy, this patient’s cancer was identified and resected at its earlier stages prior to metastasis.