Abstract
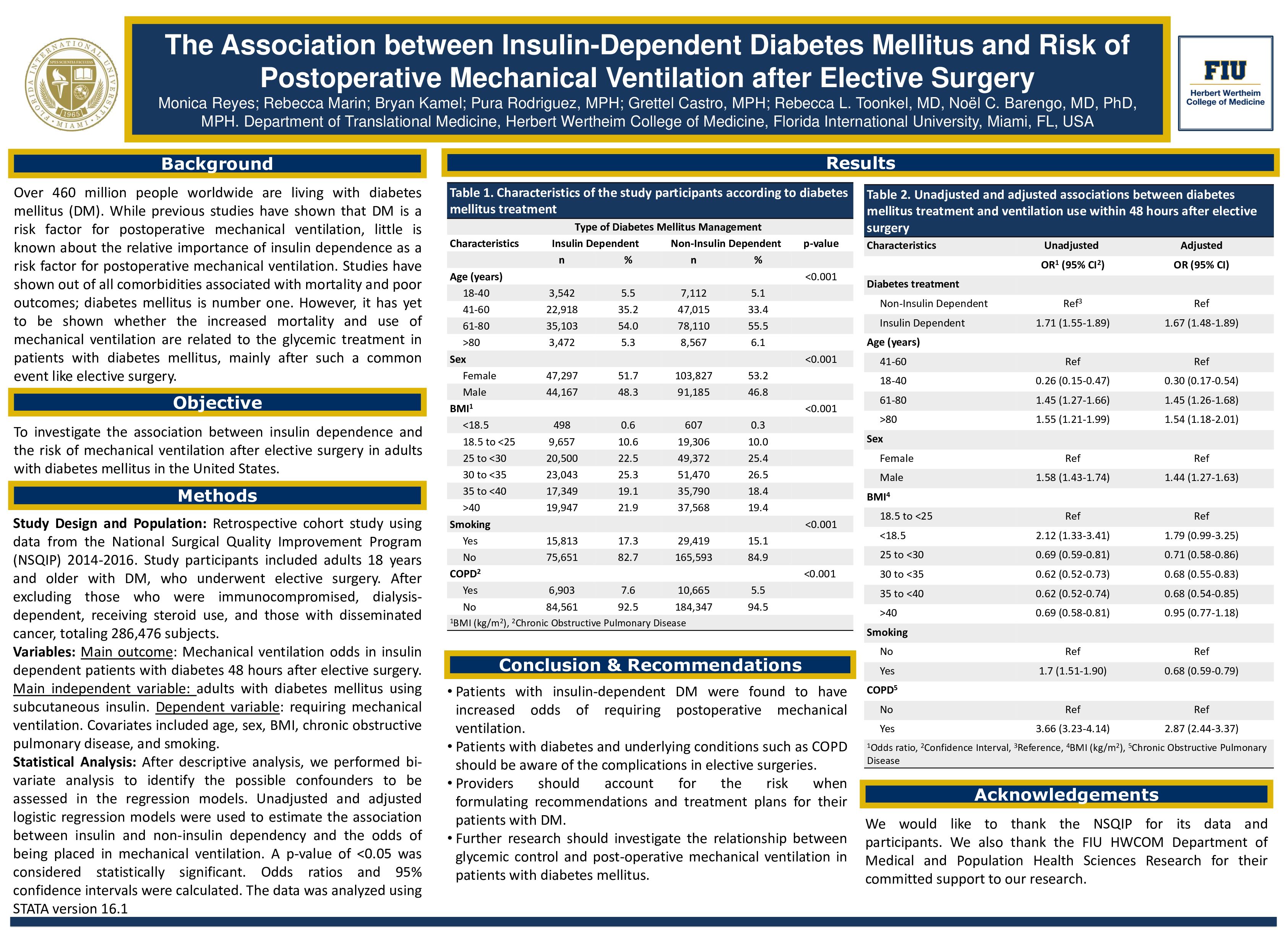
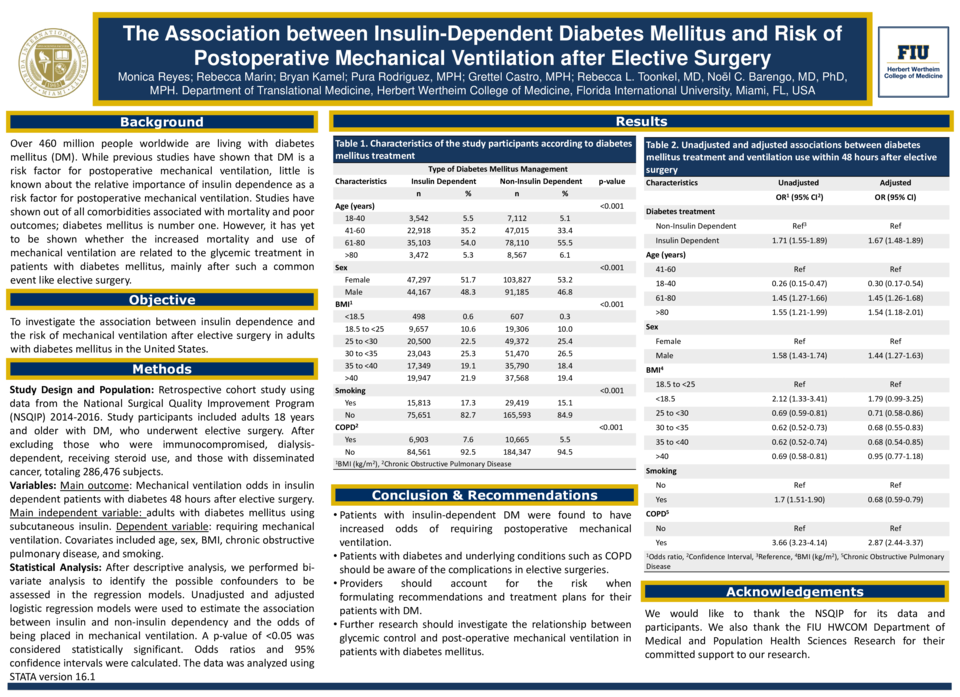
Introduction and Objective. Over 460 million people around the world are living with diabetes mellitus (DM). While previous studies have shown that DM is a risk factor for postoperative mechanical ventilation, little is known about the relative importance of insulin-dependence as a risk factor for postoperative mechanical ventilation. The objective of our study was to investigate the association between insulin dependence and the risk of mechanical ventilation after elective surgery in adults with diabetes mellitus.
Methods. This non-concurrent cohort study used data from the 2014-2016 NSQIP, which surveyed participating hospitals in the U.S. Study participants included patients 18 years and older with DM who underwent elective surgery. After excluding those who were immunocompromised, dialysis-dependent, receiving steroids for chronic conditions, and those with disseminated cancer (n=25,957), we analyzed data from 286,476 subjects. We examined the risk of post-operative mechanical ventilation at 48 hours in patients with insulin-dependent DM compared with those using oral agents alone. Covariates examined included age, sex, smoking status, and comorbidities such as hypertension and chronic obstructive pulmonary disease (COPD). Unadjusted and adjusted logistic regression analyses were used to calculate odds ratios (OR) and corresponding 95% confidence intervals (CI).
Results. Patients with insulin-dependent DM were found to be 1.67 times more likely (OR 1.67; 95% CI 1.48-1.89) to require mechanical ventilation 48 hours after elective surgery than patients with non-insulin dependent DM. Variables found to be independently associated with an increased risk for mechanical ventilation included COPD (OR 2.87; 95% CI 2.44-3.37), age >80 years (OR 1.54; 95% CI 1.18-2.01), and male sex (OR 1.44; 95% CI 1.27-1.63). Current smoking or smoking cessation within the last year was found to be protective (OR 0.68; 95% CI 0.59-0.79).
Conclusion. Insulin-dependent DM is a risk factor for mechanical ventilation after elective surgery. Providers should account for this risk when formulating recommendations and treatment plans for patients with DM. Further research should explore the relationship between glycemic control and postoperative mechanical ventilation in this patient population.
Keywords: Diabetes Mellitus; insulin; mechanical ventilation; elective surgery