Abstract
Introduction
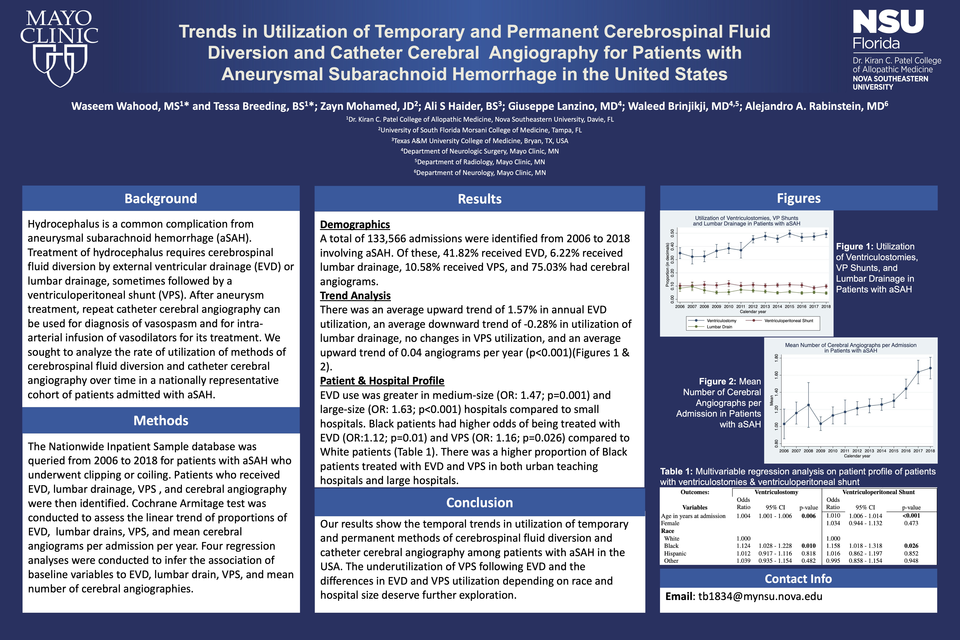
Aneurysmal subarachnoid hemorrhage (aSAH) pools blood into the subarachnoid space and may extend into the cerebrospinal fluid (CSF) ventricles, elevating intracranial pressure. This requires permanent CSF diversion achieved by external ventricular drainage (EVD) and sometimes followed by a ventriculoperitoneal shunt (VPS) if the patient develops hydrocephalus. Although predictors of EVD failure requiring VPS shunting are well-established, we sought to analyze the relationship in the utilization of the two in a nationally representative cohort.
Methods
The Nationwide Inpatient Sample database was queried from 2006 to 2018 for patients with aSAH who underwent clipping or coiling. Patients who received EVD and VPSs were also identified. Cochrane Armitage test was conducted to assess the linear trend of proportions of EVDs and VPSs per year.
Results
A total of 133,566 admissions were identified from 2006 to 2018 involving aSAH. Of these, 55,859 (41.82%) received EVDs, and 14,125 (10.58%) with VPSs. There was an average upward trend of 1.57% in EVD utilization; There was no trend seen in VPS utilization (trend: -0.06%; p=0.44).
Conclusion
Although there was an increase in the utilization of EVDs for aSAH over the years, there was an underutilization of VPSs. Previous literature demonstrates that VP shunts have higher rates of complications, and shunt dependency after aSAH raises the likelihood of morbidity and mortality. The underutilization of VPS needs to be explored further, but this phenomenon may be due to the improvement in CSF diversion management.




