Abstract
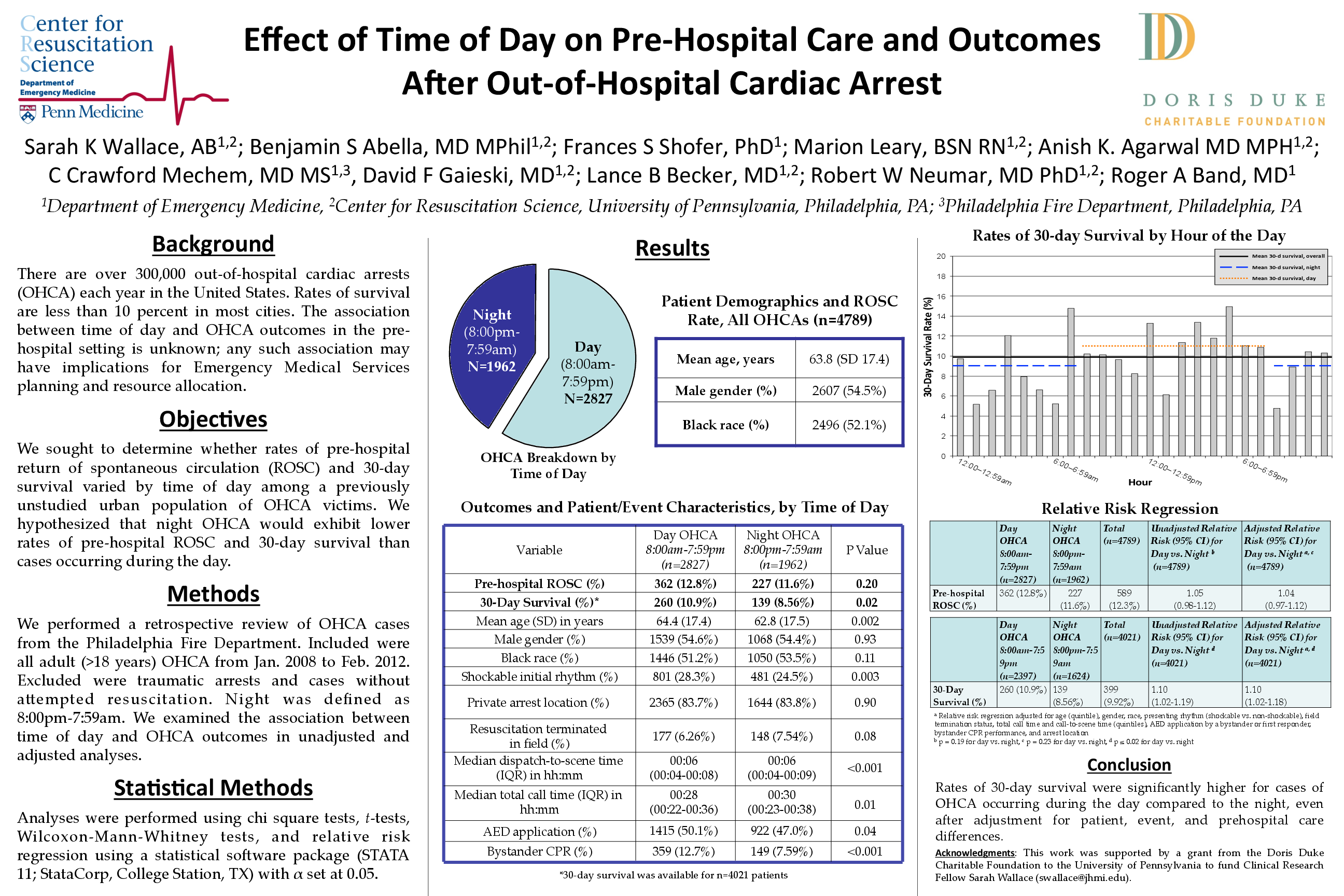
Background: There are over 300,000 out-of-hospital cardiac arrests (OHCA) each year in the United States, with rates of survival less than 10 percent in most cities. The association between time of day and OHCA outcomes in the pre-hospital setting is unknown. Any such association may have important implications for Emergency Medical Services (EMS) planning and resource allocation.
Methods and Results: We performed a retrospective review of cardiac arrest data from a large, urban EMS system. Included were all OHCA occurring in adults from January 2008 to February 2012. Excluded were traumatic arrests, patients less than 18 years of age, and cases where resuscitation measures were not performed. Day was defined as 8:00am to 7:59pm, while night was defined as 8:00pm to 7:59am. A relative risk regression model was used to evaluate the association between time of day and pre-hospital return of spontaneous circulation (ROSC) and 30-day survival, adjusting for clinically relevant predictors of survival. Among the 4,789 included cases, 1,962 (41.0%) occurred at night. Mean age was 63.8 (SD 17.4) years; males represented 54.5% of the group. Patients with an OHCA occurring at night did not have significantly lower rates of pre-hospital ROSC compared to daytime arrests (11.6% vs. 12.8%, p=0.20). However, rates of 30-day survival were significantly lower at night (8.56% vs. 10.9%, p=0.02). After adjusting for demographic factors, presenting rhythm, field termination status, duration of call, dispatch-to-scene interval, automated external defibrillator application, bystander cardiopulmonary resuscitation performance, and arrest location, 30-day survival remained significantly higher following daytime OHCA, with a relative risk of 1.10 (95% CI 1.02-1.18).
Conclusions: Rates of 30-day survival were significantly higher for cases of OHCA occurring during the day compared to the night, even after adjustment for patient, event, and pre-hospital care differences.