Abstract
Introduction
Late metastatic recurrence is a unique, unusual but well-recognized characteristic of Renal Cell Carcinoma (RCC). Late recurrence is arbitrarily defined as recurrence more than 10 years after nephrectomy for primary RCC. RCC most commonly metastasizes to the lungs, lymph nodes, bone, liver, and CNS. Cardiac metastasis from RCC without the involvement of inferior vena cava is extremely rare, and late recurrence in the heart is even more infrequent. We present a case of a patient who had late metastasis of RCC to the right ventricle 12 years after nephrectomy for primary disease.
Case Presentation
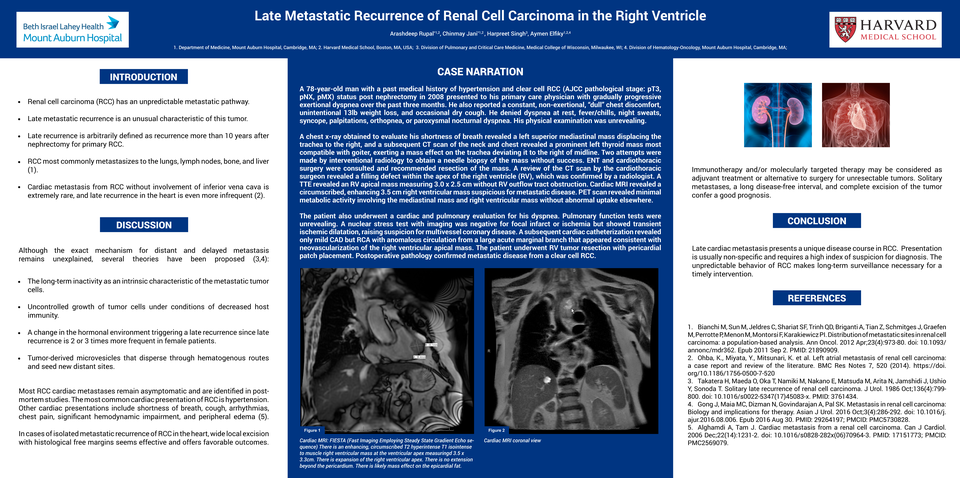
A 78-year-old man with a history of clear cell RCC (AJCC pathological stage: pT3, pNX, pMX) status post nephrectomy in 2008 presented to his primary care physician with progressive dyspnea, intermittent non-exertional chest discomfort, dry cough, and unintentional 13lb weight loss over the past 3 months. A chest x-ray revealed tracheal deviation, and a subsequent CT scan of the neck and chest revealed a large mass in the upper mediastinum and a filling defect within the apex of the right ventricle (RV). TTE revealed an RV apical mass measuring 3.0 x 2.5 cm without RV outflow tract obstruction. Cardiac MRI revealed a circumscribed, enhancing 3.5 cm right ventricular mass suspicious for metastatic disease. A nuclear stress test with imaging was negative for focal infarct or ischemia but showed transient ischemic dilatation, raising suspicion for multivessel coronary disease. A subsequent cardiac catheterization revealed only mild CAD but findings consistent with neovascularization of the right ventricular mass. PET scan revealed minimal metabolic activity involving the mediastinal mass and right ventricular mass without abnormal uptake elsewhere. The patient underwent RV tumor resection with pericardial patch placement. Postoperative pathology confirmed metastatic disease from a clear cell RCC.
Discussion
Late metastatic recurrence is an unusual but well-recognized characteristic of RCC and must be considered in patients with a previous history of RCC who present with seemingly new lesions. Although the exact mechanism for delayed metastasis remains unexplained, several theories have been proposed: the long-term inactivity as an intrinsic characteristic of the metastatic tumor cells, uncontrolled growth of tumor cells under conditions of decreased host immunity, a change in the hormonal environment triggering a late recurrence since late recurrence is 2 or 3 times more frequent in female patients, and tumor-derived microvesicles that disperse through hematogenous routes and seed new distant sites. The accepted treatment for late solitary or oligometastatic disease is wide local excision with tumor-free margins. Immunotherapy and/or molecularly targeted therapy may be considered as adjuvant treatment or alternative to surgery for unresectable tumors. Solitary metastases, a long disease-free interval, and complete excision of the tumor confer a good prognosis.
Conclusion
Late metastatic recurrence presents a unique disease course in RCC. Patients with a history of RCC should never be considered free of the risk of recurrence of this unpredictable tumor, even after complete excision of the primary tumor. The unpredictable behavior of RCC makes long-term surveillance necessary for a timely intervention.



