Abstract
BACKGROUND: Coagulation abnormalities are common in clinical practice. Causes include:
1. Vitamin K deficiency due to a) liver and gall bladder diseases, b) cystic fibrosis, c) intestinal (malabsorption or intake deficiency), d) medications and toxins, e) Vitamin K dependent clotting factor deficiency (VKCFD) (genetic). 2, Antibodies against clotting factors, e.g. factor VIII
3. Disseminated intravascular coagulation.
CASE DESCRIPTION :61-year-old female with hypertension presented with haematuria-1 day. No dysuria. History of epistaxis and melena 2 and 3 days back. No history suggestive of malabsorption or liver/gallbladder disease. No history of any trauma, intake of herbal/alternative medicines or special diet. No past, obstetric and family history significant of bleeding.
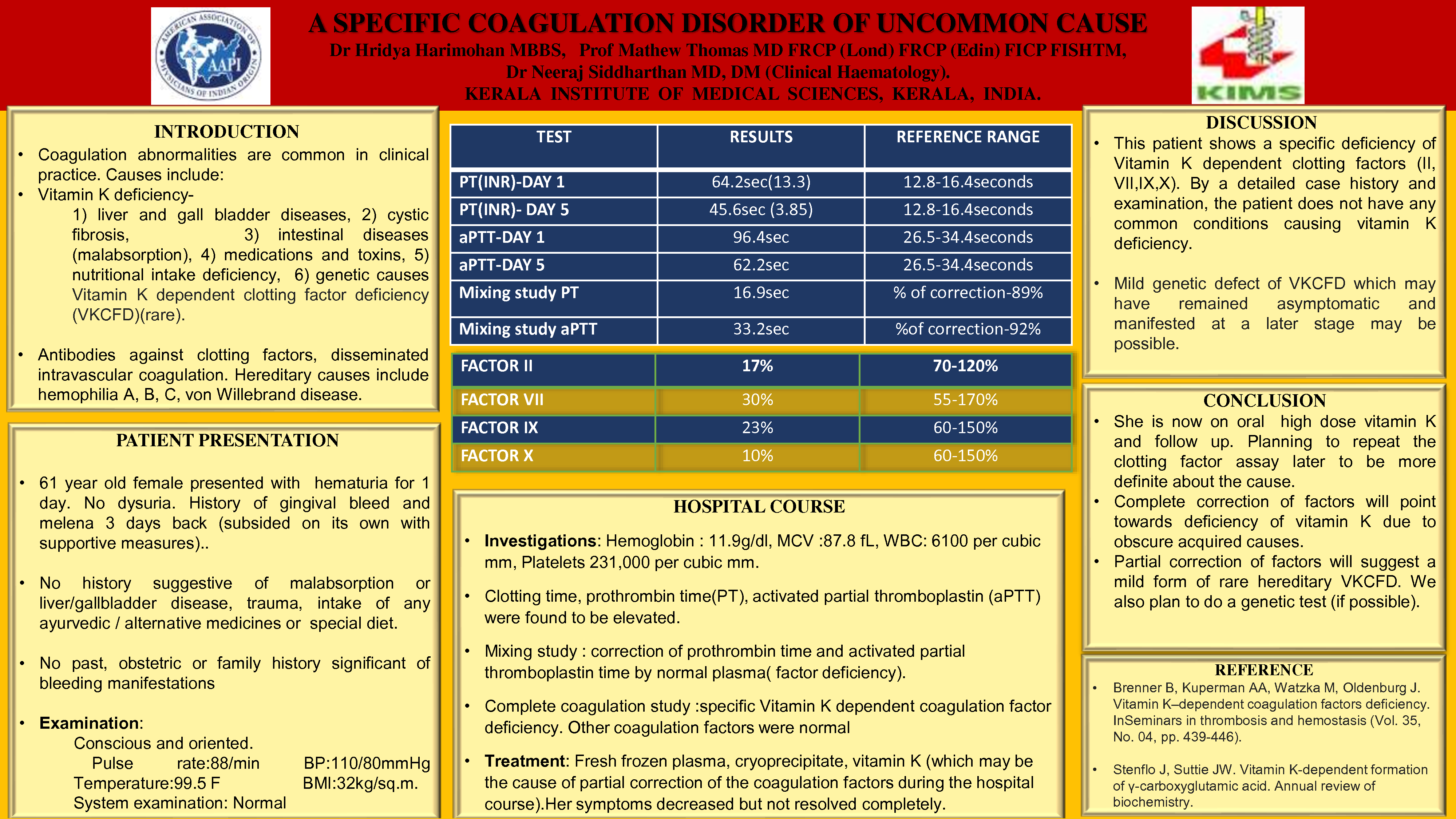
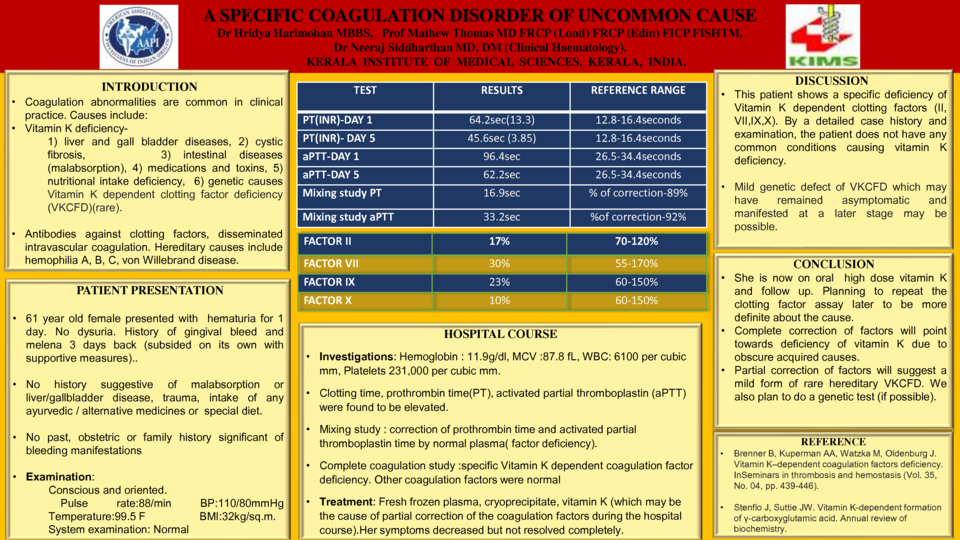
On examination, conscious and oriented. Vital signs were stable. Systemic examination: Normal. Laboratory investigations showed hemoglobin of 11.9g/dl. Clotting time (29min), prothrombin time (INR 13.3), activated partial thromboplastin (aPTT) (96.9 sec) were elevated. Mixing study showed correction of prothrombin time and activated partial thromboplastin time (aPTT) by normal plasma indicating factor deficiency. Factor assay showed deficiency of vitamin K dependent coagulation factors (II, VII, IX, X). Other factors were normal. Patient was treated with fresh frozen plasma, cryoprecipitate, vitamin K causing partial correction of the coagulation factors. Her bleeding symptoms resolved and is on follow up. INR and aPTT are still out of range.
CONCLUSION: Common causes of vitamin K deficiency were not present after detailed history, physical examination and investigations. Treatment with vitamin K improved the symptoms but was not able to correct the laboratory findings. A mild genetic defect of VKCFD which was asymptomatic and manifested now at a later stage is also considered. She is now on vitamin K and on follow up
and clotting factor assay will be done to determine the cause. • Complete correction of factors will suggest deficiency of vitamin K due to obscure acquired causes.
• Partial correction of clotting factors will suggest a mild form of rare hereditary VKCFD. We also plan to do a genetic test in the future (if possible).