Abstract
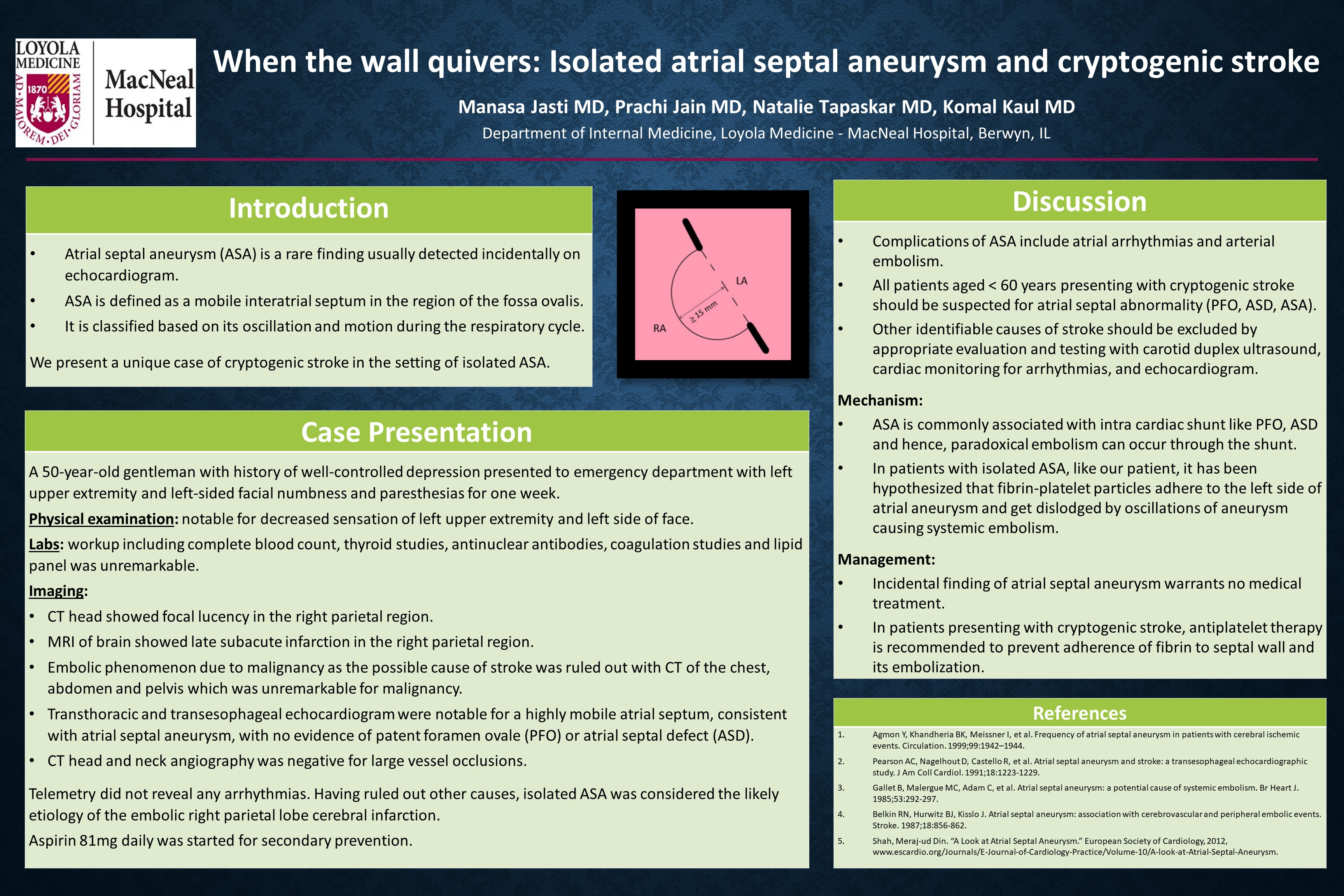
Background: Atrial septal aneurysm (ASA) is usually detected incidentally on echocardiogram. ASA is mobile interatrial septum in the region of fossa ovalis. Literature shows higher prevalence of ASA in patients who present with cryptogenic stroke, especially in age <55 years. ASA is commonly associated with intra-cardiac shunts like patent foramen ovale (PFO), atrial septal defect (ASD) and hence, paradoxical embolism can occur. However, cryptogenic stroke in the setting of isolated ASA is rare.
Aim: We present and discuss a unique case of cryptogenic stroke in the setting of isolated ASA.
Case Description: A 50-year-old gentleman with history of well-controlled depression presented to emergency department with left upper extremity and left-sided facial numbness and paresthesias for one week. Physical examination was notable for decreased sensation of left-sided face and left upper extremity. Workup including complete blood count, thyroid studies, antinuclear antibodies, coagulation studies and lipid panel was unremarkable. CT head showed focal lucency in the right parietal region. MRI of brain showed late subacute infarction in the right parietal region. Transthoracic and transesophageal echocardiogram were notable for a highly mobile atrial septum, consistent with atrial septal aneurysm, with no evidence of intra-cardiac shunt. CT head and neck angiography was negative for large vessel occlusions. Telemetry did not reveal any arrhythmias. Having ruled out other causes, isolated ASA was considered the likely etiology of the embolic stroke. Aspirin 81mg daily was started for secondary prevention.
Conclusion: All patients aged <60 years presenting with cryptogenic stroke should be suspected for atrial septal abnormality (PFO, ASD, ASA). In patients with isolated ASA, like our patient, it has been hypothesized that fibrin-platelet particles adhere to the left side of atrial aneurysm and get dislodged by oscillations of aneurysm causing systemic embolism. Incidental finding of atrial septal aneurysm warrants no treatment. When presenting with cryptogenic stroke, antiplatelet therapy is recommended.