Abstract
Introduction:
Multiple Sclerosis (MS) is an autoimmune demyelinating disorder of the central nervous system. MS affects approximately 1 million individuals in the US and 2.5 million worldwide. Patients often present with variety of symptoms such as weakness, numbness, and/or ocular disturbances. These multiple episodes are known as attacks, that occur at different time intervals, and recovery from these occur at different degrees. The McDonald Criteria revised in 2019 provides guidance to properly frame the diagnosis of MS. MS is predominately a white matter disease but can affect the cortex, gray matter and can be mistaken for seizures. This case report demonstrates a unique presentation of MS. The patient presented with a left hand spasm consisting of a contracture.
Case Description:
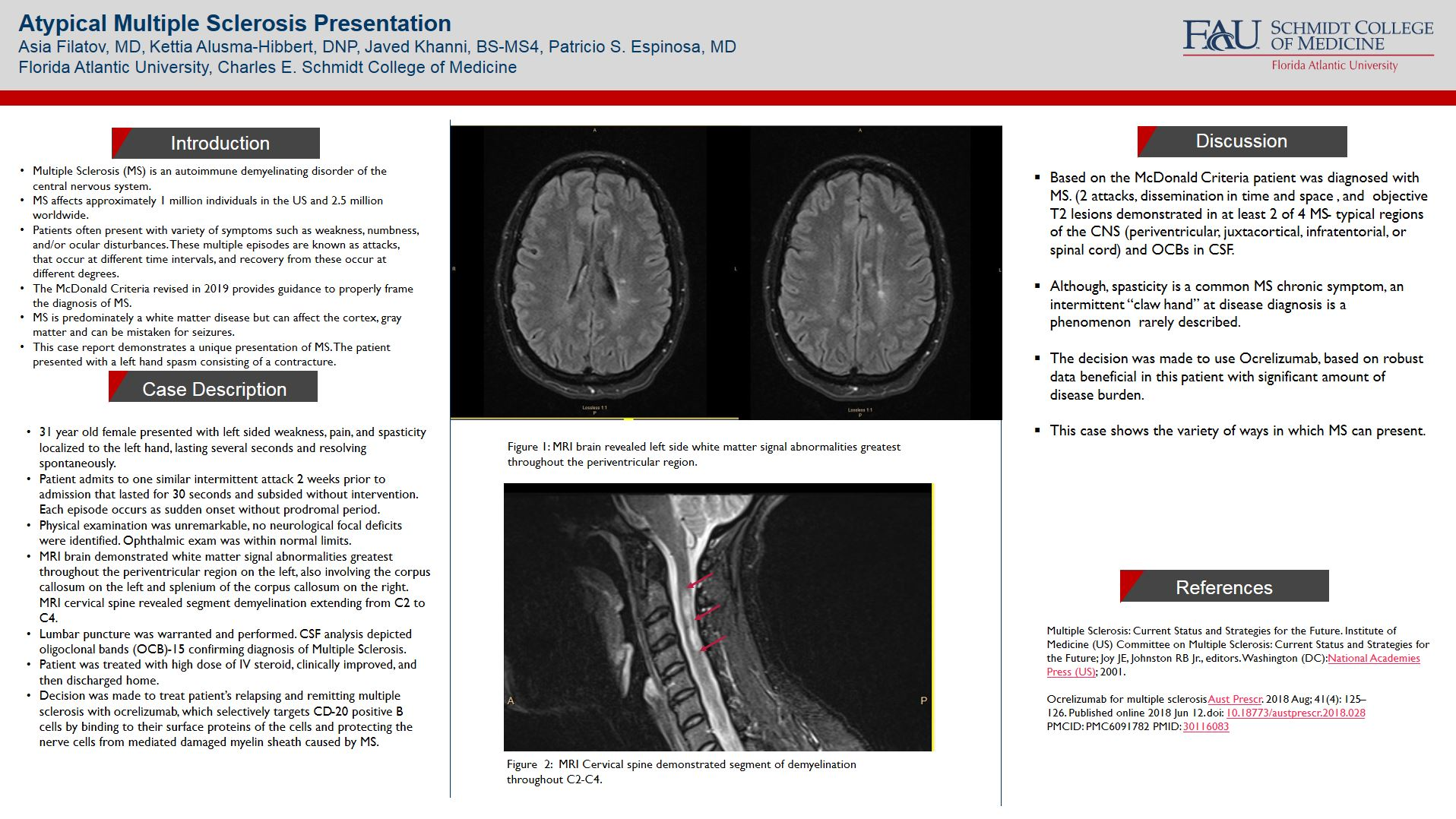
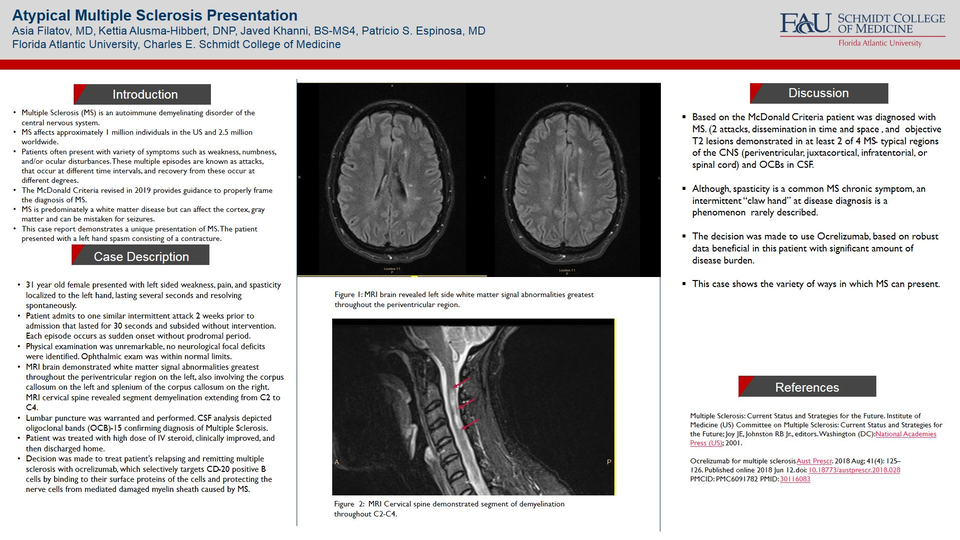
31 year old female presented with left sided weakness, pain, and spasticity localized to the left hand, lasting several seconds and resolving spontaneously. Patient admits to one similar intermittent attack 2 weeks prior to admission that lasted for 30 seconds and subsided without intervention. Each episode occurs as sudden onset without prodromal period. Physical examination was unremarkable, no neurological focal deficits were identified. Ophthalmic exam was within normal limits. MRI brain demonstrated white matter signal abnormalities greatest throughout the periventricular region on the left, also involving the corpus callosum on the left and splenium of the corpus callosum on the right. MRI cervical spine revealed segment demyelination extending from C2 to C4. Lumbar puncture was warranted and performed. CSF analysis depicted oligoclonal bands (OCB)-15 confirming diagnosis of Multiple Sclerosis. Patient was treated with high dose of IV steroid, clinically improved, and then discharged home. Decision was made to treat patient’s relapsing and remitting multiple sclerosis with ocrelizumab, which selectively targets CD-20 positive B cells by binding to their surface proteins of the cells and protecting the nerve cells from mediated damaged myelin sheath caused by MS.
Discussion:
Based on the McDonald Criteria patient was diagnosed with MS. (2 attacks, dissemination in time and space , and objective T2 lesions demonstrated in at least 2 of 4 MS- typical regions of the CNS (periventricular, juxtacortical, infratentorial, or spinal cord) and OCBs in CSF. Although, spasticity is a common MS chronic symptom, an intermittent “claw hand” at disease diagnosis is a phenomenon rarely described.The decision was made to use Ocrelizumab, based on robust data beneficial in this patient with significant amount of disease burden. This case shows the variety of ways in which MS can present.
References:
- Multiple Sclerosis: Current Status and Strategies for the Future. Institute of Medicine (US) Committee on Multiple Sclerosis: Current Status and Strategies for the Future; Joy JE, Johnston RB Jr., editors. Washington (DC): National Academies Press (US); 2001.
- Ocrelizumab for multiple sclerosis Aust Prescr. 2018 Aug; 41(4): 125–126. Published online 2018 Jun 12. doi: 10.18773/austprescr.2018.028 PMCID: PMC6091782 PMID: 30116083.