Abstract
Objectives: Manual VMAT planning techniques for radiotherapy have been FDA approved since 2008. Recent automated VMAT planning and delivery techniques have been developed to standardize methods and improve the efficiency of planning and delivery. Here we report an early clinical experience with automated VMAT (HyperArcTM) for brain metastases radiosurgery including all targets in a single isocenter.
Methods: The included patients were treated with automated VMAT SRS or 5 fraction SBRT using HyperArcTM during Oct 2017 and May 2018-March 2019. Included tumors had no prior surgery or radiation for local treatment and had available MRI follow-up imaging. Doses were prescribed volumetrically such that 99-100% of the target received 100% of the dose. The most commonly prescribed doses were 18-20 Gy in 1 fraction and 30 Gy in 5 fractions. The dose was prescribed to the edge of the GTV with zero PTV margin. Local failure was defined as a 25% increase in tumor diameter on follow-up contrasted MRI or pathologic confirmation of tumor recurrence. A 25% increase in tumor diameter followed by subsequent stabilization or improvement on follow-up imaging was classified as locally controlled. This was to account for the treatment effect of both radiotherapy or immunotherapy. Locally controlled tumors were censored at the time of last MRI follow-up, death, or whole brain radiation for distant brain failure. Significant CNS toxicity was defined per CTCAE definition as any Grade 3 or higher toxicity. LC and CNS toxicity were evaluated by the Kaplan-Meier (KM) method.
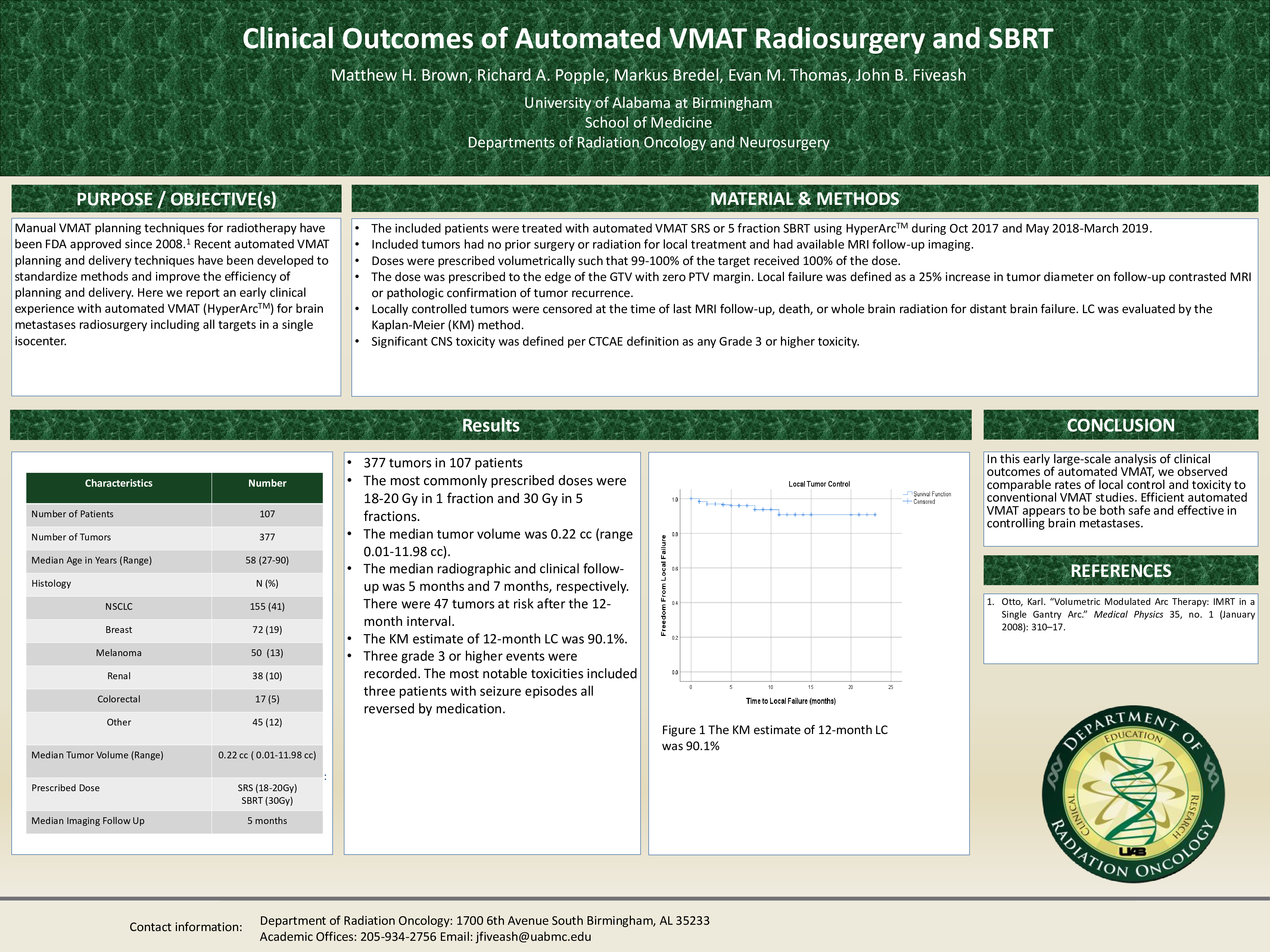
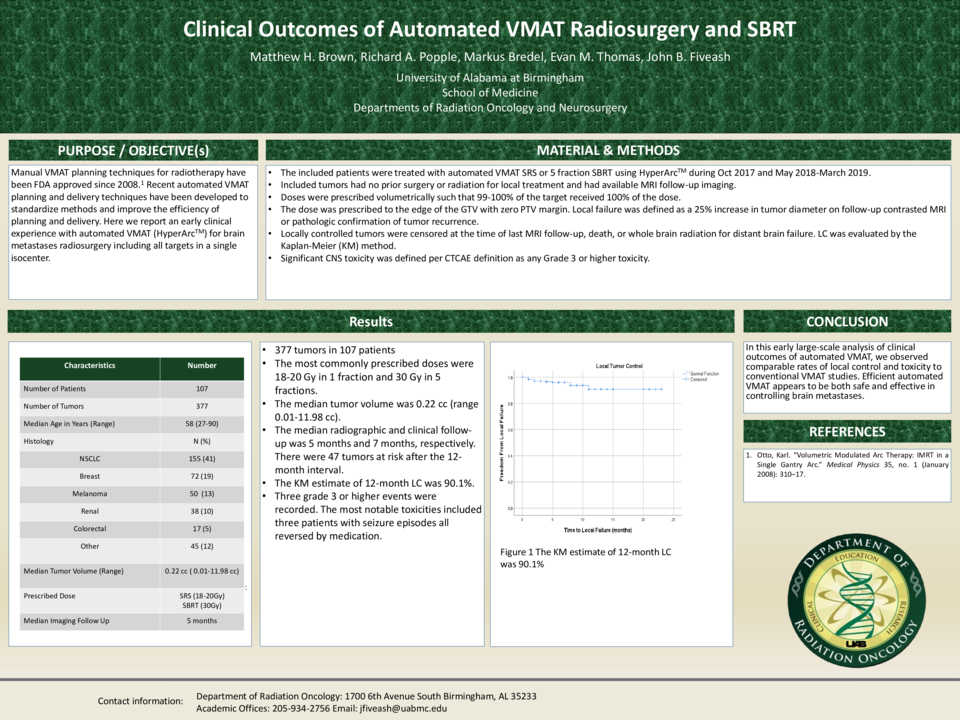
Results: A total of 377 tumors in 107 patients of varying histologies were included in the analysis. The tumor types included 41% NSCLC, 19% breast, 13% melanoma, and 27% other. The median tumor volume was 0.22 cc (range 0.01-11.98 cc). The median radiographic and clinical follow-up was 5 months and 7 months, respectively. There were 47 tumors at risk after the 12-month interval. The KM estimate of 12-month LC was 90.1%. Three grade 3 or higher events were recorded. The most notable toxicities included three patients with seizure episodes all reversed by medication.
Conclusion: In this early large-scale analysis of clinical outcomes of automated VMAT, we observed comparable rates of local control and toxicity to conventional VMAT studies. Efficient automated VMAT appears to be both safe and effective in controlling brain metastases.