Abstract
Introduction: Hypofractionated stereotactic radiosurgery plans for tumors in and adjacent to the brainstem are an option. Treatment efficacy and complications of this paradigm are incompletely understood.
Objectives: To review the results of the treatment of brainstem lesions with hypofractionated stereotactic radiosurgery.
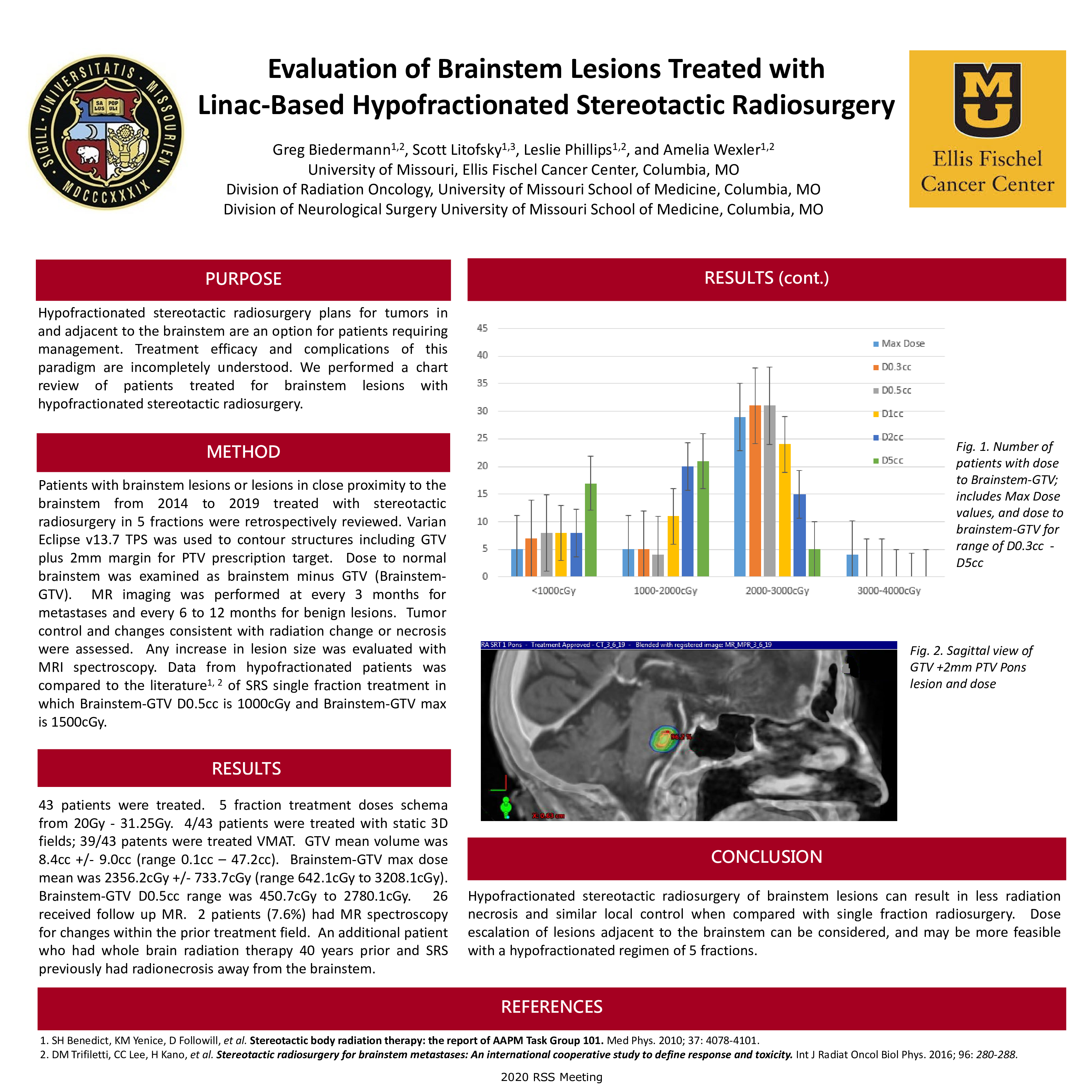
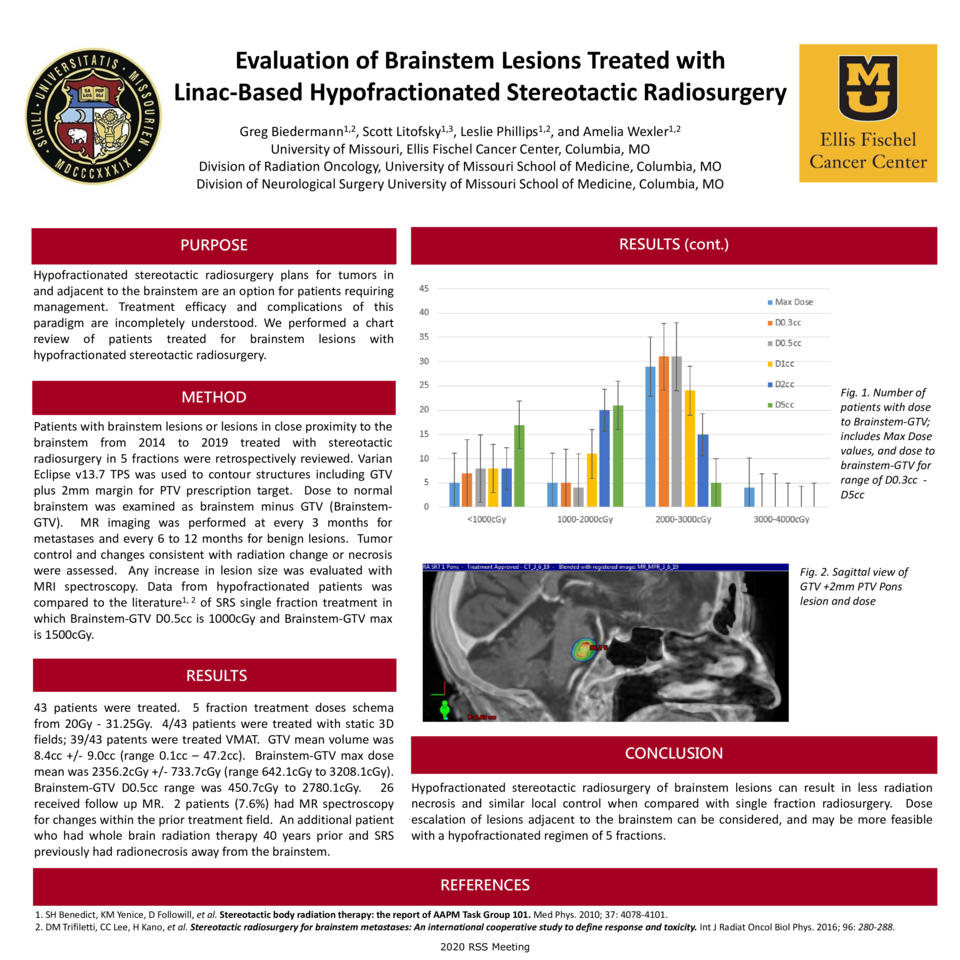
Methods: Patients with brainstem lesions or lesions in close proximity to the brainstem from 2014 to 2019 treated with stereotactic radiosurgery in 5 fractions were retrospectively reviewed. Varian Eclipse v13.7 TPS was used to contour structures including GTV plus 2mm margin for PTV prescription target. Dose to normal brainstem was examined as brainstem minus GTV (Brainstem-GTV). MR imaging was performed at every 3 months for metastases and every 6 to12 months for benign lesions. Tumor control and changes consistent with radiation change or necrosis were assessed. Any increase in lesion size was evaluated with MRI spectroscopy. Data from hypofractionated patients was compared to the literature1, 2 of SRS single fraction treatment in which Brainstem-GTV D0.5cc is 1000cGy and Brainstem-GTV max is 1500cGy.
Results: 43 patients were treated. 5 fraction treatment doses schema from 20Gy - 31.25Gy. 4/43 patients were treated with static 3D fields; 39/43 patients were treated VMAT. GTV mean volume was 8.4cc +/- 9.0cc (range 0.1cc – 47.2cc). Brainstem-GTV max dose mean was 2356.2cGy +/- 733.7cGy (range 642.1cGy to 3208.1cGy). Brainstem-GTV D0.5cc range was 450.7cGy to 2780.1cGy. 26 received follow up MR. 2 patients (7.6%) had MR spectroscopy for changes within the prior treatment field. An additional patient who had whole-brain radiation therapy 40 years prior and SRS previously had radionecrosis away from the brainstem.[LNS1].
Conclusions: Hypofractionated stereotactic radiosurgery of brainstem lesions can result in less radiation necrosis and similar local control when compared with single fraction radiosurgery. Dose escalation of lesions adjacent to the brainstem can be considered and may be more feasible with a hypofractionated regimen of 5 fractions.