Abstract
INTRODUCTION
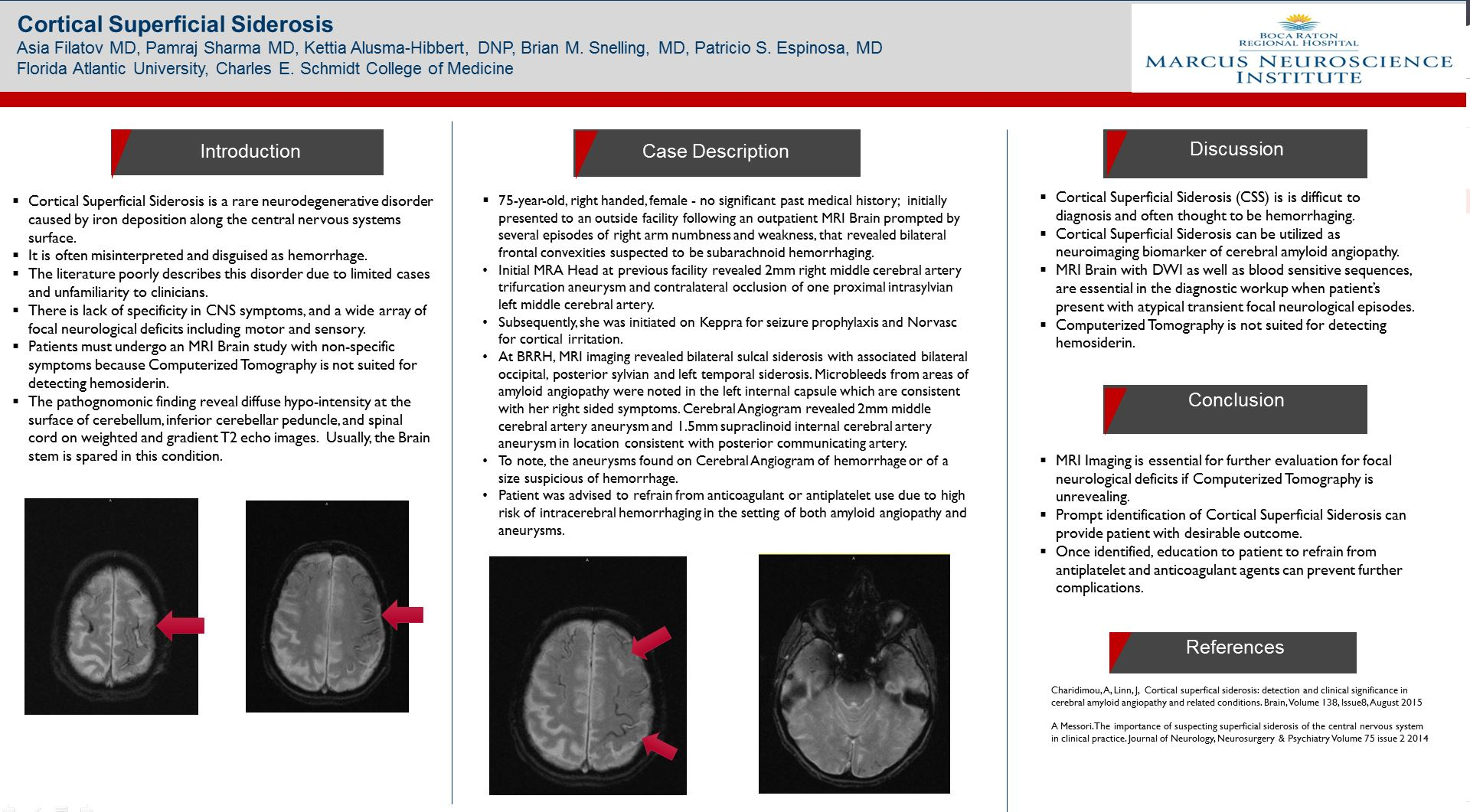
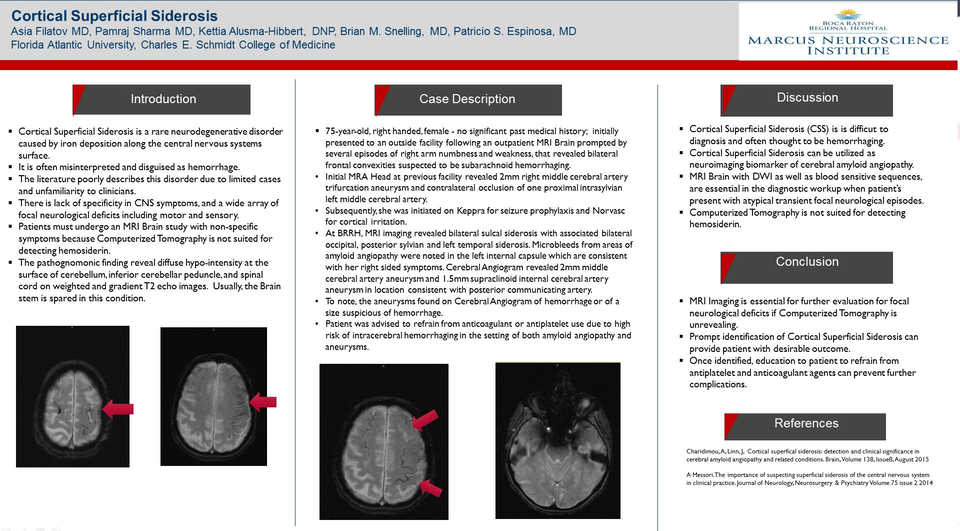
Cortical Superficial Siderosis is a rare neurodegenerative disorder caused by iron deposition along the central nervous systems surface. It is often misinterpreted and disguised as hemorrhage. The literature poorly describes this disorder due to limited cases and unfamiliarity to clinicians. There is lack of specificity in CNS symptoms, and a wide array of focal neurological deficits including motor and sensory. Patients must undergo an MRI Brain study with non-specific symptoms because Computerized Tomography is not suited for detecting hemosiderin. The pathognomonic finding reveal diffuse hypo-intensity at the surface of cerebellum, inferior cerebellar peduncle, and spinal cord on weighted and gradient T2 echo images. Usually, the Brain stem is spared in this condition.
CASE REPORT
75-year-old, right handed, female - no significant past medical history; initially presented to an outside facility following an outpatient MRI Brain prompted by several episodes of right arm numbness and weakness, that revealed bilateral frontal convexities suspected to be subarachnoid hemorrhaging.
Initial MRA Head at previous facility revealed 2mm right middle cerebral artery trifurcation aneurysm and contralateral occlusion of one proximal intrasylvian left middle cerebral artery. Subsequently, she was initiated on Keppra for seizure prophylaxis and Norvasc for cortical irritation. At BRRH, MRI imaging revealed bilateral sulcal siderosis with associated bilateral occipital, posterior sylvian and left temporal siderosis. Microbleeds from areas of amyloid angiopathy were noted in the left internal capsule which are consistent with her right sided symptoms. Cerebral Angiogram revealed 2mm middle cerebral artery aneurysm and 1.5mm supraclinoid internal cerebral artery aneurysm in location consistent with posterior communicating artery. To note, the aneurysms found on Cerebral Angiogram of hemorrhage or of a size suspicious of hemorrhage. Patient was advised to refrain from anticoagulant or antiplatelet use due to high risk of intracerebral hemorrhaging in the setting of both amyloid angiopathy and aneurysms.
DISCUSSION
Cortical Superficial Siderosis (CSS) is is difficut to diagnosis and often thought to be hemorrhaging. Cortical Superficial Siderosis can be utilized as neuroimaging biomarker of cerebral amyloid angiopathy. MRI Brain with DWI as well as blood sensitive sequences, are essential in the diagnostic workup when patient’s present with atypical transient focal neurological episodes. Computerized Tomography is not suited for detecting hemosiderin.
CONCLUSION
MRI Imaging is essential for further evaluation for focal neurological deficits if Computerized Tomography is unrevealing. Prompt identification of Cortical Superficial Siderosis can provide patient with desirable outcome. Once identified, education to patient to refrain from antiplatelet and anticoagulant agents can prevent further complications.
REFERENCES
Charidimou, A, Linn, J, Cortical superfical siderosis: detection and clinical significance in cerebral amyloid angiopathy and related conditions. Brain, Volume 138, Issue8, August 2015
A Messori.The importance of suspecting superficial siderosis of the central nervous system in clinical practice. Journal of Neurology, Neurosurgery & Psychiatry Volume 75 issue 2 2014