Abstract
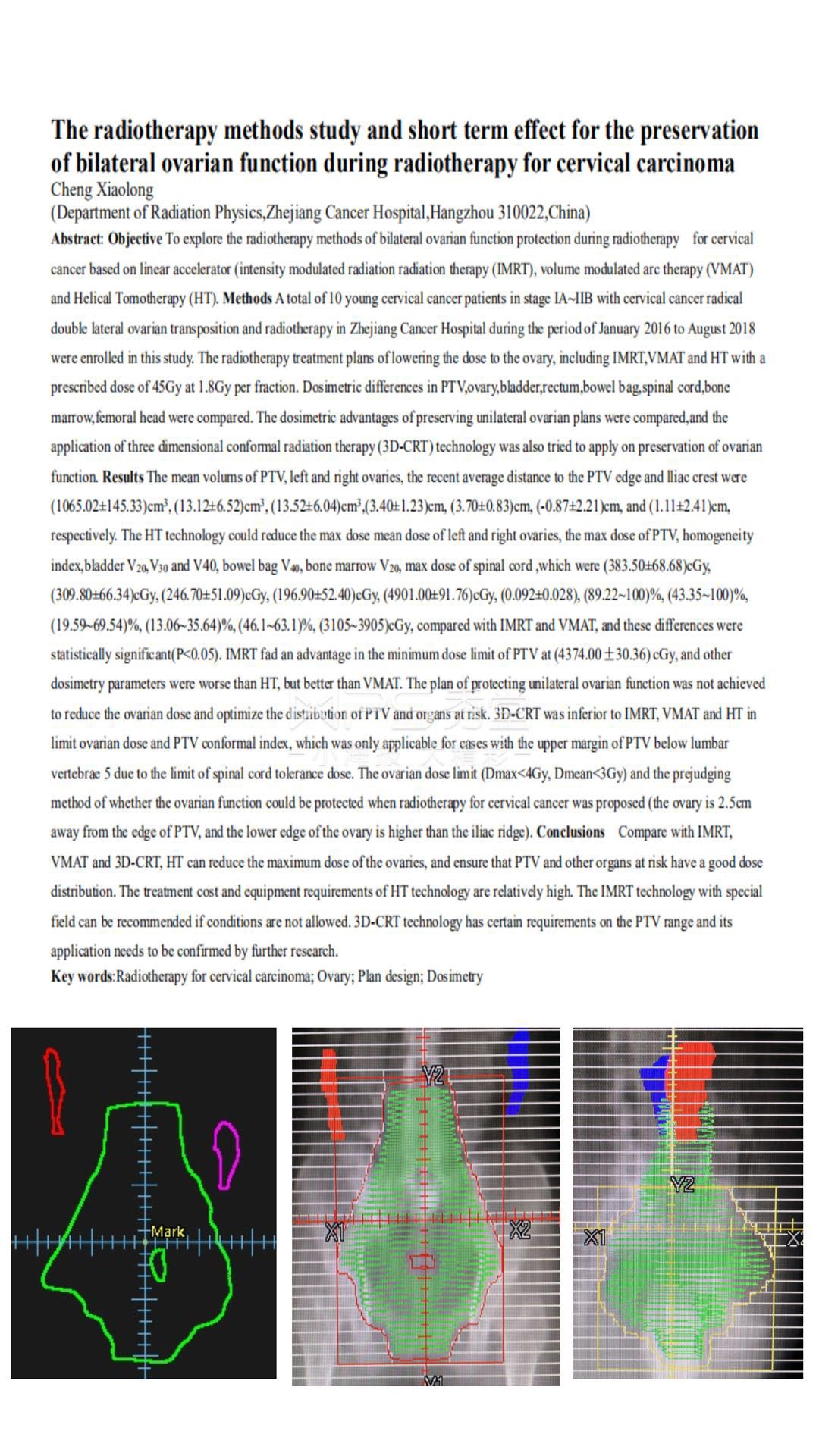
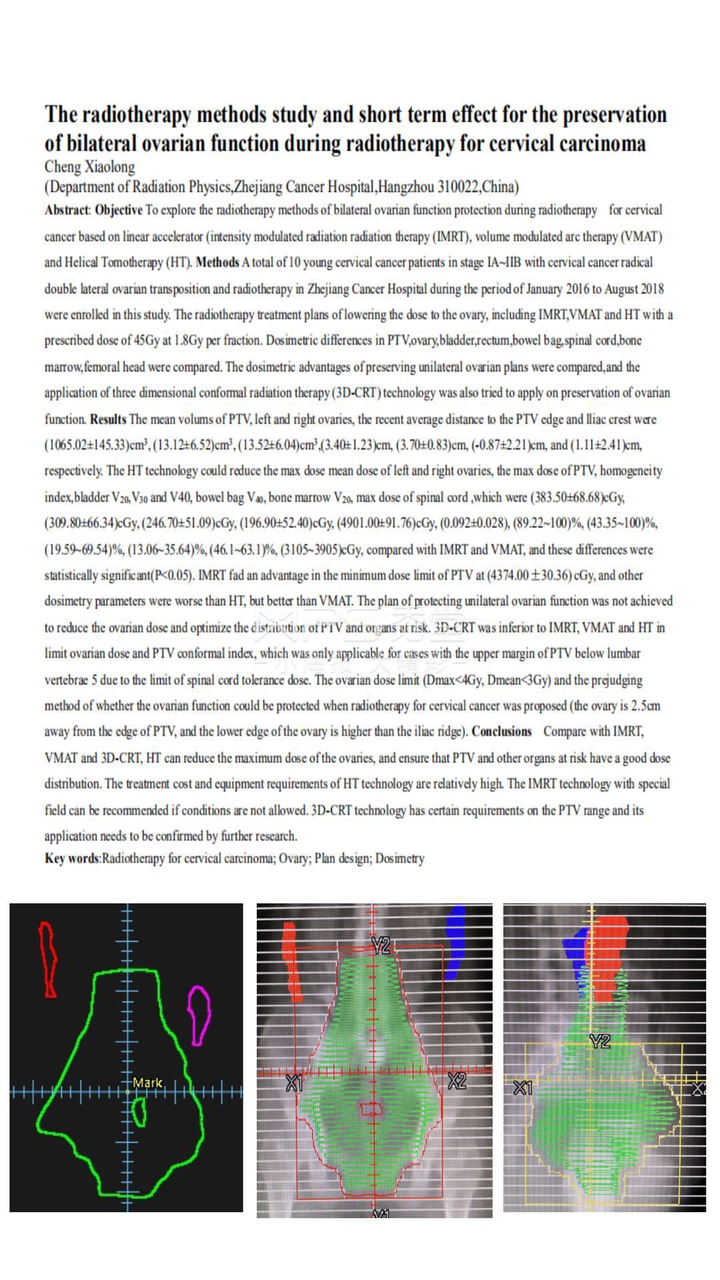
Objective To explore the radiotherapy methods of bilateral ovarian function protection during radiotherapy for cervical cancer based on linear accelerator (intensity modulated radiation radiation therapy (IMRT), volume modulated arc therapy (VMAT) and Helical Tomotherapy (HT). Methods A total of 10 young cervical cancer patients in stage IA~IIB with cervical cancer radical double lateral ovarian transposition and radiotherapy in Zhejiang Cancer Hospital during the period of January 2016 to August 2018 were enrolled in this study. The radiotherapy treatment plans of lowering the dose to the ovary, including IMRT,VMAT and HT with a prescribed dose of 45Gy at 1.8Gy per fraction. Dosimetric differences in PTV,ovary,bladder,rectum,bowel bag,spinal cord,bone marrow,femoral head were compared. The dosimetric advantages of preserving unilateral ovarian plans were compared,and the application of three dimensional conformal radiation therapy (3D-CRT) technology was also tried to apply on preservation of ovarian function. Results The mean volums of PTV, left and right ovaries, the recent average distance to the PTV edge and lliac crest were (1065.02±145.33)cm3, (13.12±6.52)cm3, (13.52±6.04)cm3,(3.40±1.23)cm, (3.70±0.83)cm, (-0.87±2.21)cm, and (1.11±2.41)cm,
respectively. The HT technology could reduce the max dose mean dose of left and right ovaries, the max dose of PTV, homogeneity index,bladder V20,V30 and V40, bowel bag V40, bone marrow V20, max dose of spinal cord ,which were (383.50±68.68)cGy, (309.80±66.34)cGy, (246.70±51.09)cGy, (196.90±52.40)cGy, (4901.00±91.76)cGy, (0.092±0.028), (89.22~100)%, (43.35~100)%, (19.59~69.54)%, (13.06~35.64)%, (46.1~63.1)%, (3105~3905)cGy, compared with IMRT and VMAT, and these differences were statistically significant(P<0.05). IMRT fad an advantage in the minimum dose limit of PTV at (4374.00±30.36) cGy, and other dosimetry parameters were worse than HT, but better than VMAT. The plan of protecting unilateral ovarian function was not achieved to reduce the ovarian dose and optimize the distribution of PTV and organs at risk. 3D-CRT was inferior to IMRT, VMAT and HT in limit ovarian dose and PTV conformal index, which was only applicable for cases with the upper margin of PTV below lumbar vertebrae 5 due to the limit of spinal cord tolerance dose. The ovarian dose limit (Dmax<4Gy, Dmean<3Gy) and the prejudging method of whether the ovarian function could be protected when radiotherapy for cervical cancer was proposed (the ovary is 2.5cm away from the edge of PTV, and the lower edge of the ovary is higher than the iliac ridge). Conclusions Compare with IMRT, VMAT and 3D-CRT, HT can reduce the maximum dose of the ovaries, and ensure that PTV and other organs at risk have a good dose distribution. The treatment cost and equipment requirements of HT technology are relatively high. The IMRT technology with special field can be recommended if conditions are not allowed. 3D-CRT technology has certain requirements on the PTV range and its application needs to be confirmed by further research.