Abstract
Trauma is the most common cause of upper extremity amputations, and tend to occur in a younger, predominantly male population. Given that upper extremity function, particularly thumb function, is crucial for activities of daily living, the management of these injuries has significant impact on long term pain, disability, and overall physical/psychosocial outcomes.
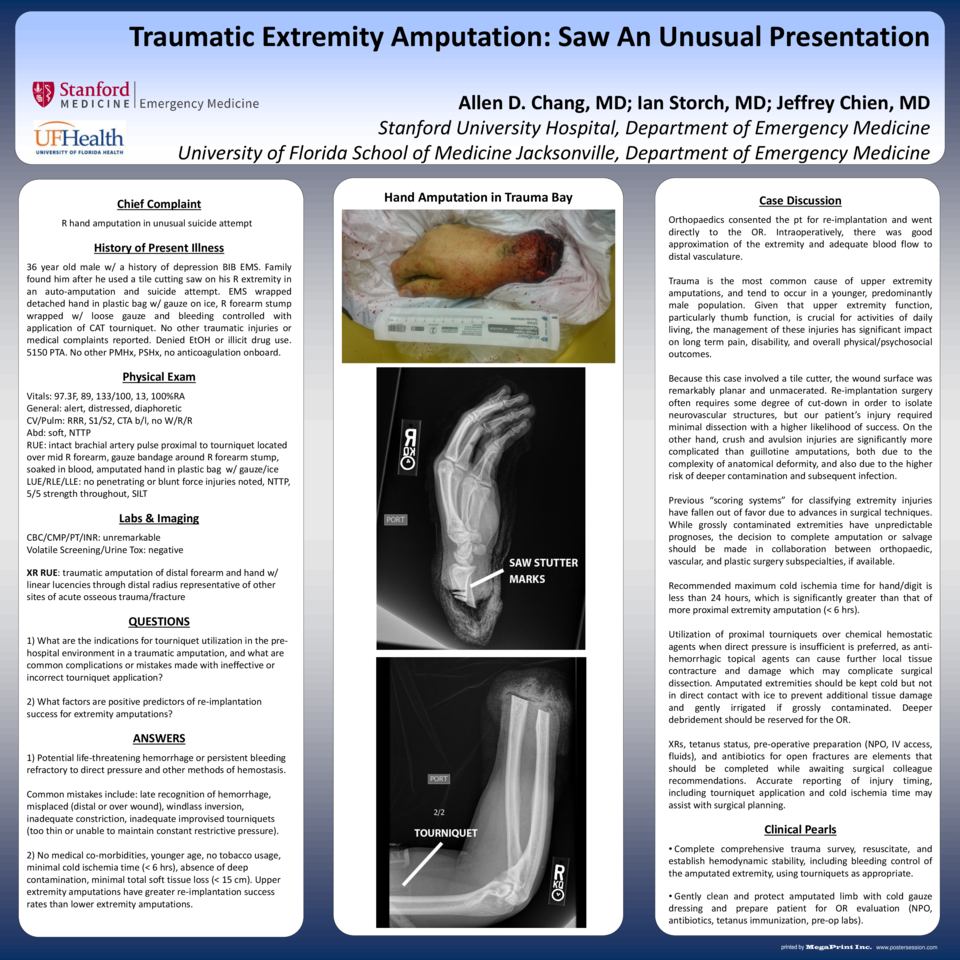
Because this case involved a tile cutter, the wound surface was remarkably planar and unmacerated. Re-implantation surgery often requires some degree of cut-down in order to isolate neurovascular structures, but our patient’s injury required minimal dissection with a higher likelihood of success. On the other hand, crush and avulsion injuries are significantly more complicated than guillotine amputations, both due to the complexity of anatomical deformity, and also due to the higher risk of deeper contamination and subsequent infection.
Previous “scoring systems” for classifying extremity injuries have fallen out of favor due to advances in surgical techniques. While grossly contaminated extremities have unpredictable prognoses, the decision to complete amputation or salvage should be made in collaboration between orthopaedic, vascular, and plastic surgery subspecialties, if available.
Recommended maximum cold ischemia time for hand/digit is less than 24 hours, which is significantly greater than that of more proximal extremity amputation (< 6 hrs).
Utilization of proximal tourniquets over chemical hemostatic agents when direct pressure is insufficient is preferred, as anti-hemorrhagic topical agents can cause further local tissue contracture and damage which may complicate surgical dissection. Amputated extremities should be kept cold but not in direct contact with ice to prevent additional tissue damage and gently irrigated if grossly contaminated. Deeper debridement should be reserved for the OR.
XRs, tetanus status, pre-operative preparation (NPO, IV access, fluids), and antibiotics for open fractures are elements that should be completed while awaiting surgical colleague recommendations. Accurate reporting of injury timing, including tourniquet application and cold ischemia time may assist with surgical planning.




