Abstract
Objectives
To assess the impact of evolution of radiotherapy (RT) regimens and image-guidance (IGRT) protocols on local control (LC) for T2N0 glottic cancer treated with partial-laryngeal IMRT.
Methods
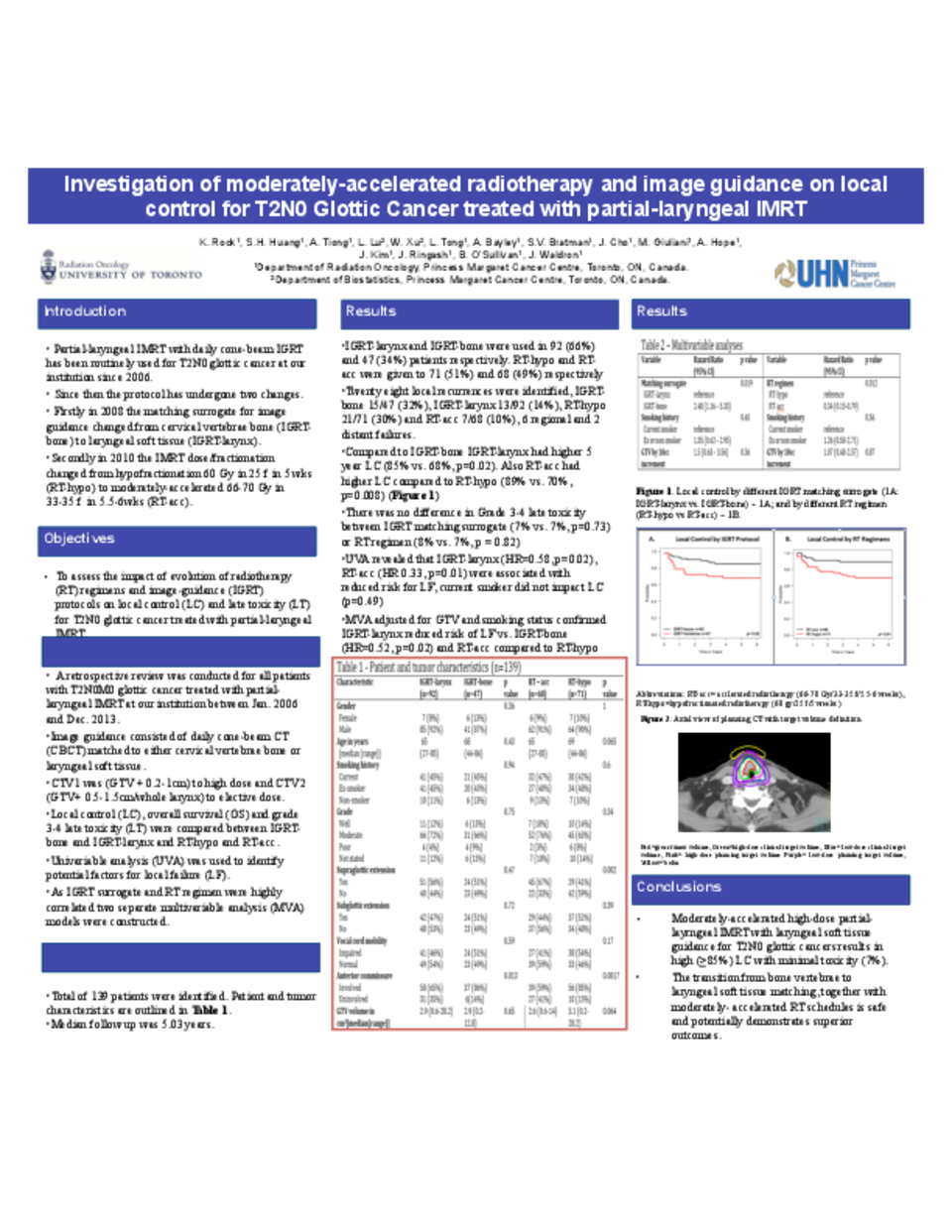
All T2N0 glottic cancer treated with IMRT in 2006-2013 were reviewed. GTV was delineated based on endoscopic/radiological findings. Higher-dose CTV was (GTV +0.2-1cm); lower-dose CTV was GTV + 0.5 – 1.5 cm/whole larynx. PTV was CTV + 0.5 cm circumferentially with 0.5 - 1cm superior-inferiorly. RT regimens evolved from hypofractionated IMRT (RT-hypo, 60 Gy in 25 fractions over 5 weeks [60 Gy/25f/5w]) to moderately-accelerated IMRT (RT-acc, 66-70 Gy/33-35f/5.5-6w) since 2010. The matching surrogate for IGRT was changed from cervical bone (IGRT-bone) to laryngeal tissue (IGRT-larynx) since 2008. LC by RT-hypo vs RT-acc and IGRT-bone vs IGRT-larynx were compared. Multivariable analysis (MVA) assessed the impact of IGRT surrogate and RT regimen on local failure (LF), separately.
Results
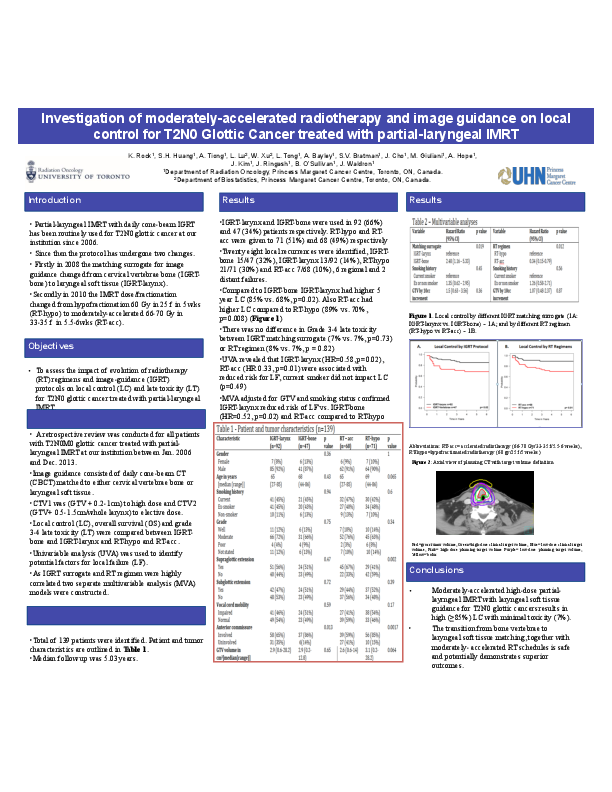
A total of 139 patients were identified. Median follow-up was 5.03 years. Twenty eight local (IGRT-bone: 15/47, IGRT-larynx: 13/92), 6 regional, 2 distant failures were identified. Higher LC was observed for IGRT-larynx (n=92) vs IGRT-bone (n=47) (85% vs 68%, p=0.02), and RT-acc (n=71) vs RT-hypo (n=68) (89% vs 70%, p=0.008). MVA adjusted for GTV and smoking status confirmed that IGRT-larynx vs IGRT-larynx (HR=0.40, 95% CI 1.2-5.3, p=0.02) and RT-acc vs RT-hypo (HR 0.34, 0.15-0.79, p=0.012) both reduced risk of LF.
Conclusions
This single-institutional cohort study shows a high LC (≥85%) for T2N0 glottic cancer following moderately-accelerated partial laryngeal IMRT (66-70 Gy/33-35f/5.5-6w) with daily laryngeal-matching IGRT.