Abstract
Purpose
To prospectively evaluate the impact of DIBH on ipsilateral right lung V20Gy during locoregional radiation (RT) for right-sided breast cancer patients in whom the free breathing (FB) V20Gy was ≥ 30%.
Materials & Methods
A prior study identified that DIBH produced a clinically meaningful reduction in pulmonary dose in comparison to FB during loco-regional RT for right-sided breast cancer (mean reduction in right lung V20Gy of 7.8%). This prompted a policy change at the Tom Baker Cancer Centre. Commencing in March 2016, all right-sided locoregional breast cancer patients with a FB ipsilateral lung V20Gy ≥ 30% had a DIBH treatment plan developed prior to compromising on internal mammary chain (IMC) lymph node coverage. If the absolute difference in lung V20Gy was ≥ 5% between plans, the DIBH plan was used for treatment. We prospectively recorded the FB and DIBH V20Gy values for patients impacted by this policy change.
Results
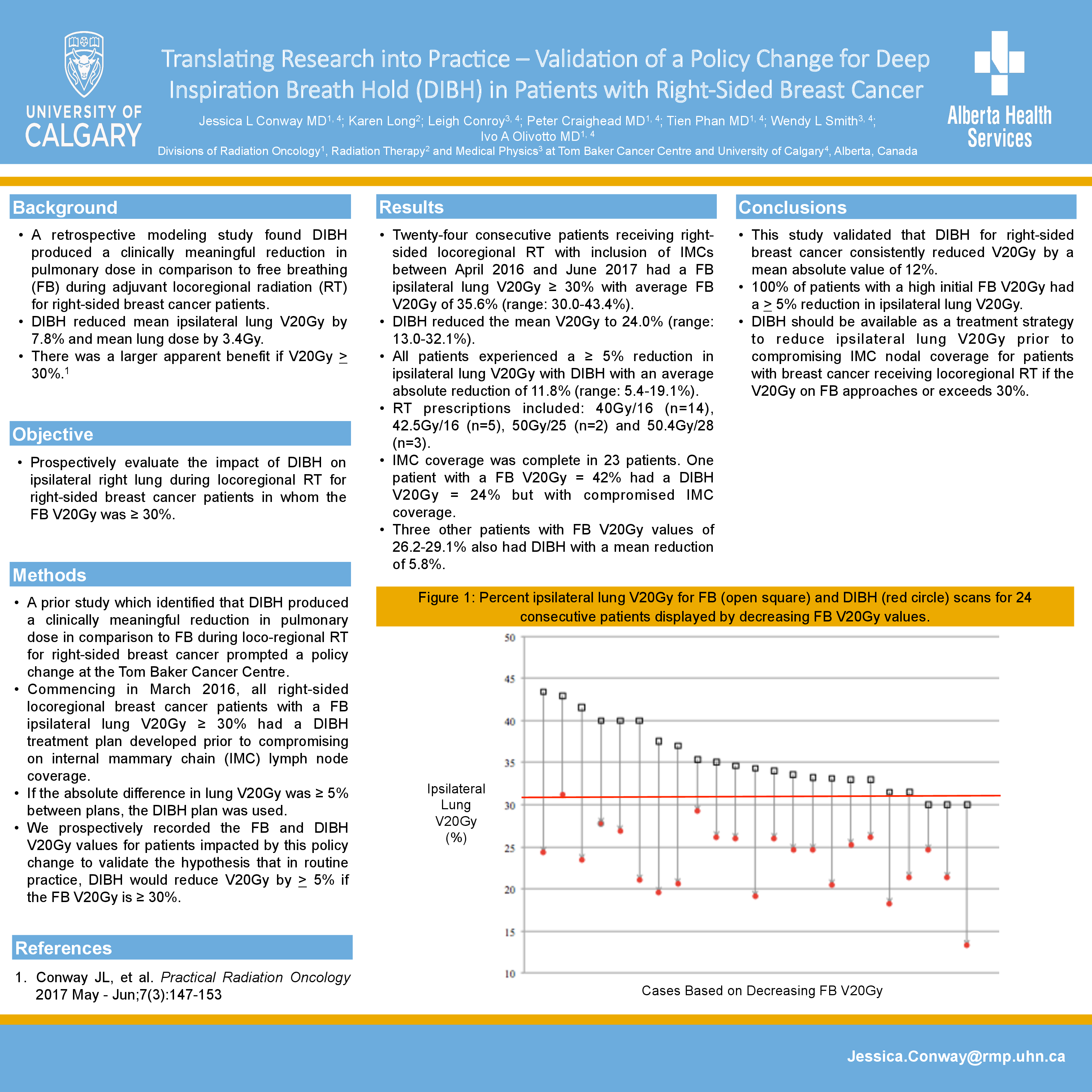
Fourteen patients receiving right-sided locoregional RT with inclusion of IMCs between April 2016 and February 2017 had a FB ipsilateral lung V20Gy ≥ 30% with an average FB V20Gy of 34% (range: 30-43%). DIBH reduced the mean V20Gy to 23% (range: 13-29%). All patients experienced a ≥ 5% reduction in ipsilateral lung V20Gy with DIBH with an average absolute reduction of 11% (range: 5-19%). RT prescriptions included 40Gy/16 (n=8), 42.5Gy/16 (n=3), 50Gy/25 (n=2) and 50.4Gy/28 (n=1). Three other patients with FB V20Gy values of 26-29% also had DIBH with a mean reduction of 6%. IMC coverage was not compromised for any patient.
Conclusions
Prospective evaluation confirmed that DIBH for right-sided breast cancer reduced the right lung V20Gy. 100% of patients with a high initial FB V20Gy had a > 5% reduction in ipsilateral lung V20Gy. DIBH should be available as a treatment strategy to reduce ipsilateral lung V20Gy prior to compromising IMC nodal coverage for patients with breast cancer receiving locoregional RT if the V20Gy on FB approaches or exceeds 30%.