Abstract
Purpose/Objective(s)
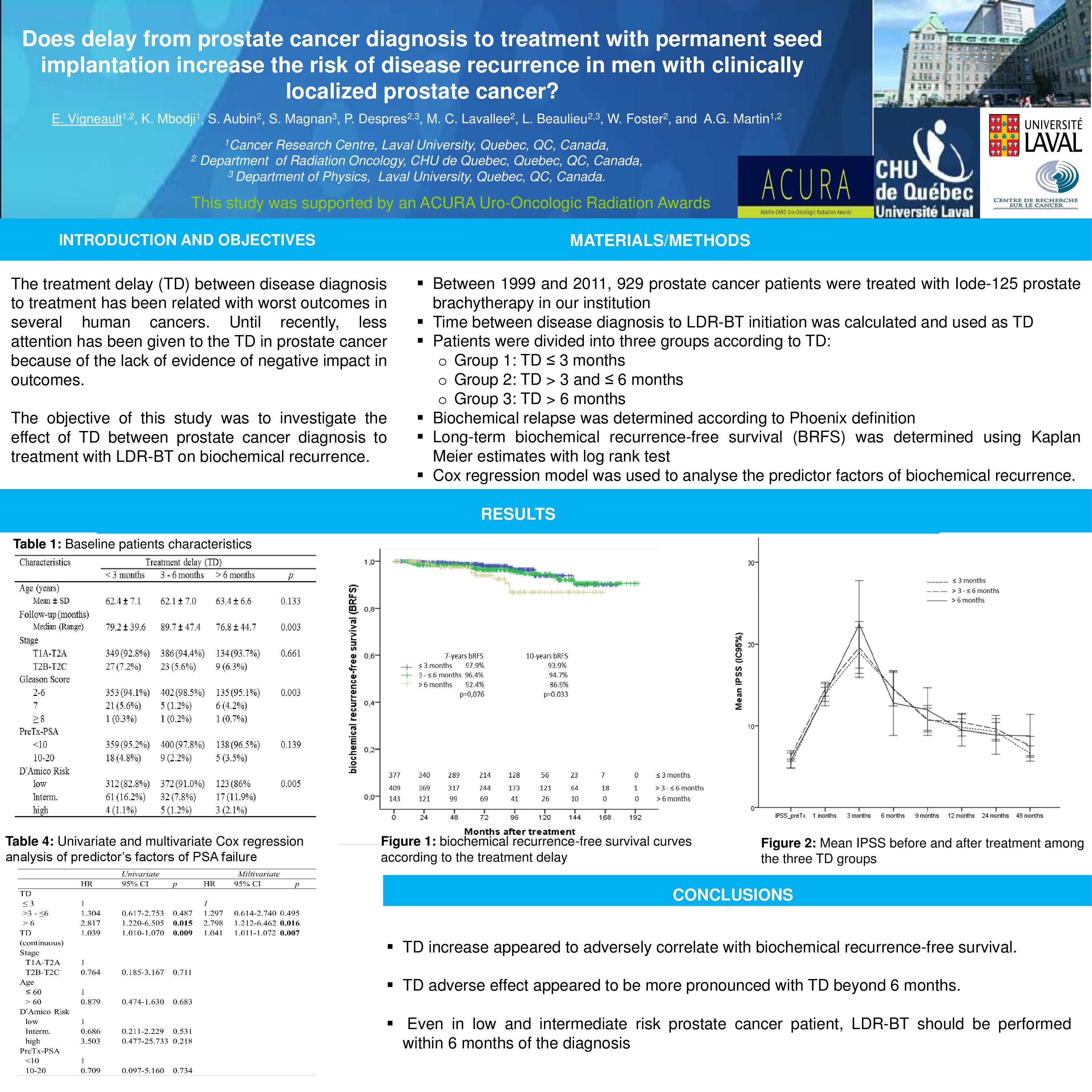
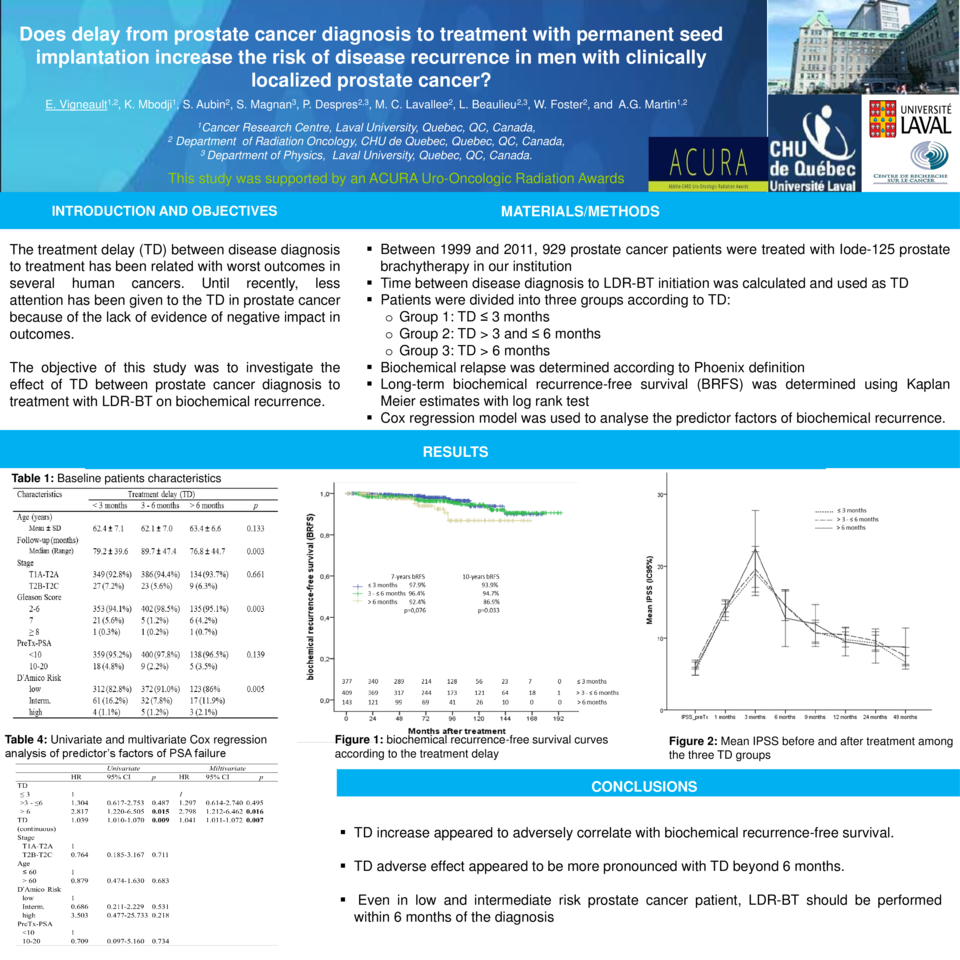
To investigate the effect of treatment delay between prostate cancer diagnosis to treatment with low-dose-rate brachytherapy (LDR-BT) on biochemical recurrence.
Materials/Methods
929 prostate cancer patients diagnosed with localized prostate cancer were treated with Iode-125 prostate brachytherapy between 1999 and 2011. The treatment delay (TD) between disease diagnosis to LDR-BT treatment was reported. Patients were divided into three groups according to TD: TD ≤3 months, 3-6 months and >6 months. Biochemical relapse was determined according to Phoenix definition. Long-term biochemical recurrence-free survival (BRFS) was determined using Kaplan Meier estimates with log rank test. Cox regression model was used to analyse the predictor factors of biochemical recurrence.
Results
Mean age and median follow-up were 62 years and 80 months, respectively. The percentage of patients with low and intermediate D’Amico risk group was 38.7%, 46.1%, 15.2% and 55.5%, 29%, 15.5% in TD ≤3 months, 3-6 months and >6 months groups (p=0.005), respectively. The 7-and 10-year BRFS for the entire cohort was 96.4% and 93.5%, respectively. When stratified by TD, the BRFS rates at 7-, 10-year were 97.9%, 96.4%, 92.4% (p=0.076) and 93.9%, 94.7% 86.9% (p=0.033) for TD ≤3 months, 3-6 months and >6 months, respectively. In univariate and multivariate Cox analysis, only TD, both categorical and continuous was a significant predictor of biochemical recurrence. Indeed, Compared to patients with TD ≤3 months, TD between 3-6 months was not associated with biochemical recurrence, while TD beyond 6 months was significantly associated with an increased risk of biochemical recurrence (HR: 2.817; 95%CI 1.220-6.505; p=0.015 and HR: 2.839; 95%CI 0.1.227-6.569; p=0.015 for univariate and multivariate, respectively). When TD was used as continuous variable, we found HR: 1.039; 95%CI 1.010-1.070; p=0.009 and HR: 1.041; 95%CI 1.011-1.072; p=0.007 for univariate and multivariate, respectively.
Conclusion
These findings showed that TD increase appeared to adversely correlate with biochemical recurrence-free survival and this effect was more pronounced with TD beyond 6 months. Even in low and intermediate risk prostate cancer patient, LDR-BT should be performed within 6 months of the diagnosis.