Abstract
Background
Infants with prenatally diagnosed congenital heart disease often necessitate multidisciplinary collaboration in the delivery room and early postnatal period. Precise and accurate assessment of the infant immediately following delivery and throughout the resuscitation is critical for optimizing outcomes. Some conditions may require aggressive intervention and procedures in the immediate period after birth. While fetal echocardiogram is a useful diagnostic tool, there are anatomic and functional variations that are not always able to be fully elucidated antenatally. Potential challenges that may be encountered in the delivery room can be explored through simulation, and then anticipated and prepared for in advance.
Educational Goal
A scheduled cesarean section was planned for a full-term infant with hypoplastic left heart syndrome with restrictive atrial septum. This patient was felt to be at high risk for needing emergent balloon atrial septostomy. Simulation was utilized to explore the logistics of the delivery, including the resuscitation plan, necessary personnel, communication amongst the multidisciplinary team, and transportation to the cardiac catheterization lab.
Approach to Addressing the Goal
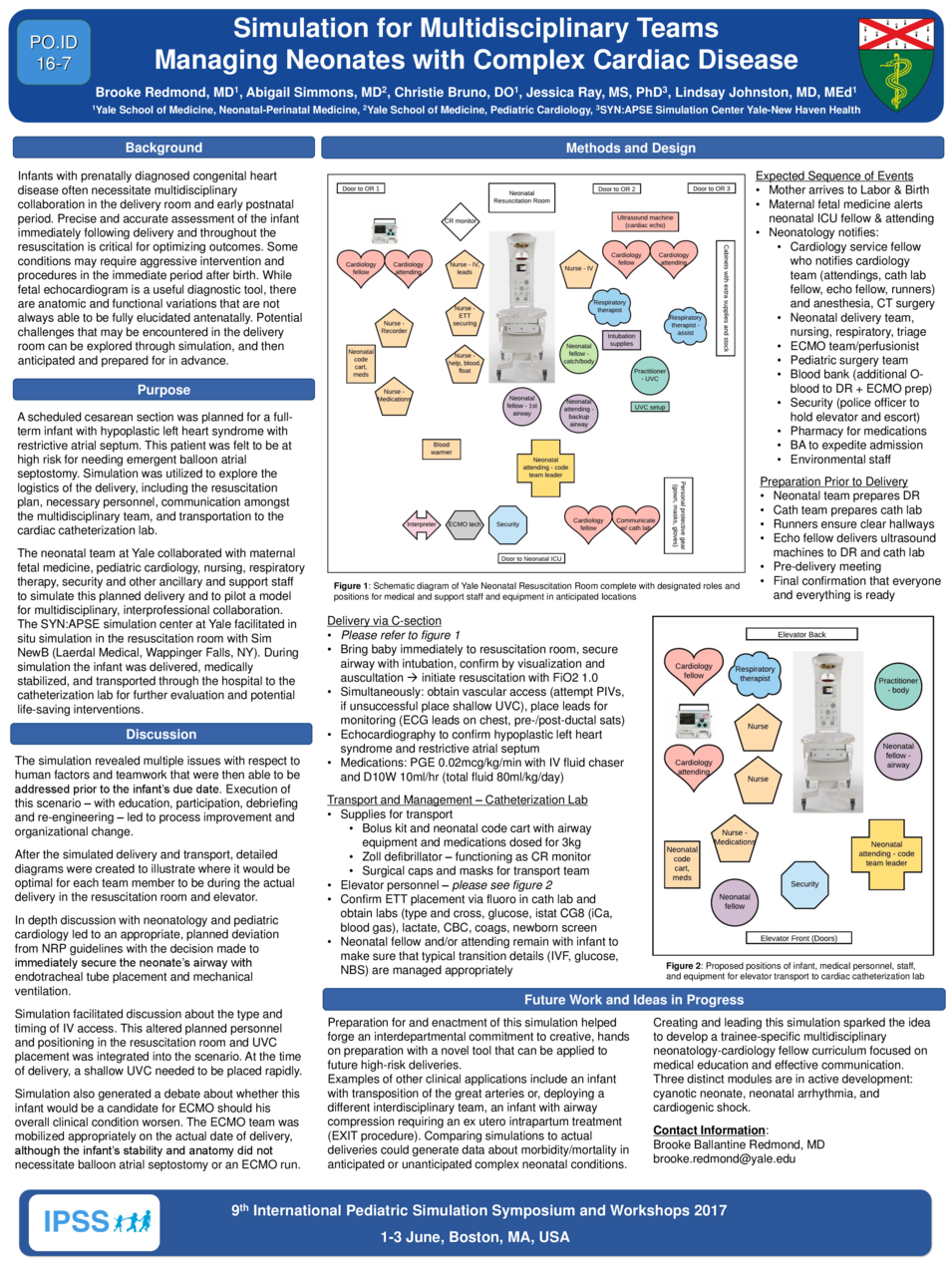
The neonatal team at Yale collaborated with maternal fetal medicine, pediatric cardiology, nursing, respiratory therapy, security and other ancillary and support staff to simulate this planned delivery and to pilot a model for multidisciplinary, interprofessional collaboration. The SYN:APSE simulation center at Yale facilitated in situ simulation in the resuscitation room with Sim NewB (Laerdal Medical, Wappinger Falls, NY). During simulation the infant was delivered, medically stabilized, and transported through the hospital to the catheterization lab for further evaluation and potential life-saving interventions.
The simulation revealed multiple issues with respect to human factors and teamwork that were then able to be addressed prior to the infant’s due date. Execution of this scenario – with education, participation, debriefing and re-engineering – led to process improvement and organizational change. After the simulated delivery and transport, detailed diagrams were created to illustrate where it would be optimal for each team member to be during the actual delivery in the resuscitation room and elevator. In depth discussion with neonatology and pediatric cardiology led to an appropriate, planned deviation from NRP guidelines with the decision made to immediately secure the neonate’s airway with endotracheal tube placement and mechanical ventilation. Simulation facilitated discussion about the type and timing of IV access and whether this infant would be a candidate for ECMO should his overall clinical condition worsen.
Creating and leading this simulation sparked the idea to develop a trainee-specific multidisciplinary neonatology-cardiology fellow curriculum focused on medical education and effective communication. It also forged an interdepartmental commitment to creative, hands on preparation, a novel tool that can be applied to other high-risk deliveries in the future. The hope is that this unique approach will lead to improved morbidity and mortality in anticipated or unanticipated complex neonatal conditions.



