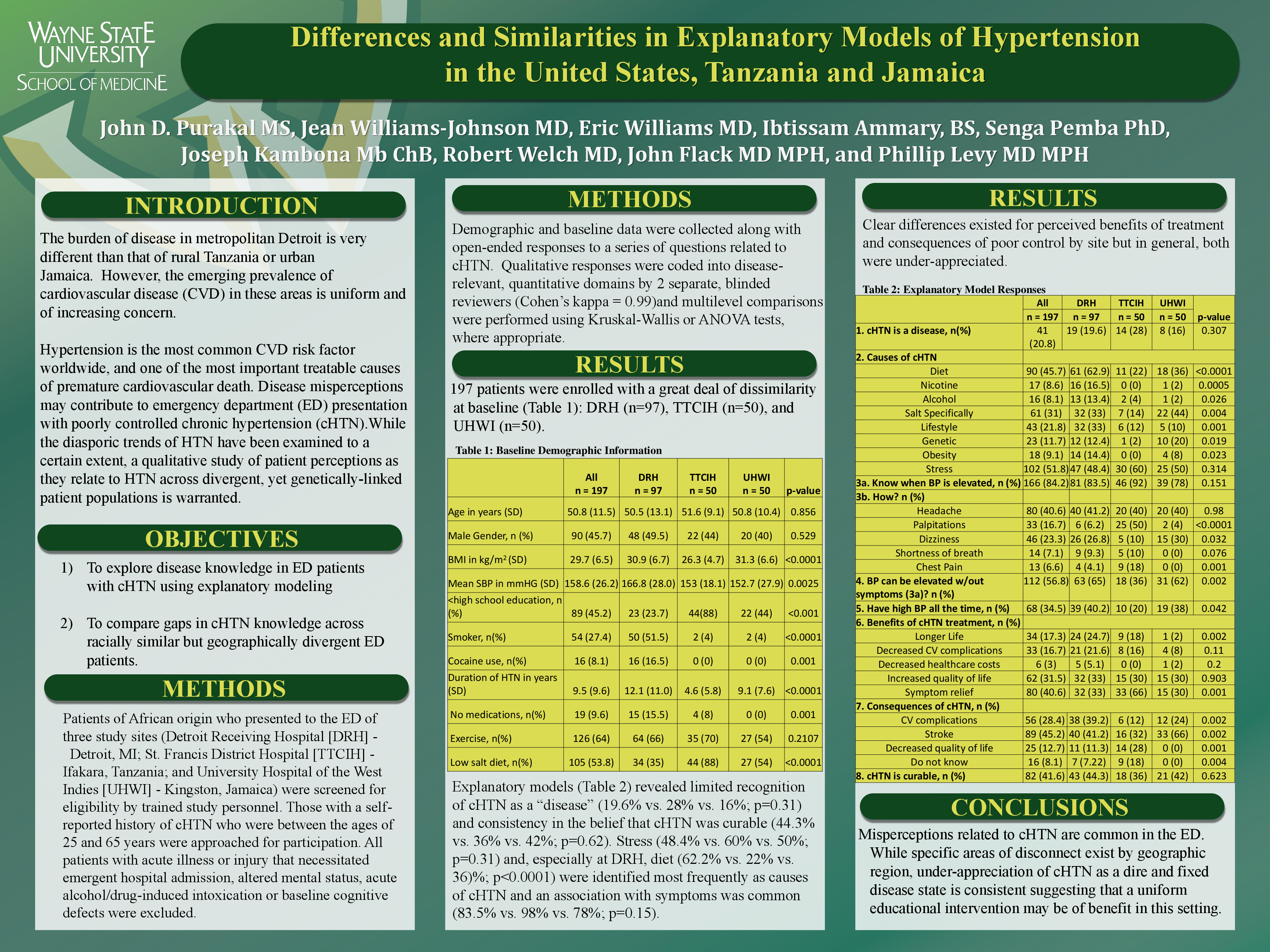
Differences and Similarities in Explanatory Models of Hypertension in the United States, Tanzania and Jamaica
Abstract
Our objectives are to explore disease knowledge in ED patients with cHTN using explanatory modeling; and to compare gaps in cHTN knowledge across racially similar but geographically divergent ED patients.
Background: Disease misperceptions may contribute to emergency department (ED) presentation with poorly controlled chronic hypertension (cHTN).
METHODS: ED patients of African origin with cHTN were recruited from 3 sites: Detroit Receiving Hospital (DRH - Detroit, MI), the Tanzanian Training Center for International Health (TTCIH – Ifakara, TZ) and University Hospital of the West Indies (UHWI – Kingston, JA). Demographic and baseline data were collected along with open-ended responses to a series of questions related to cHTN. Qualitative responses were coded into disease-relevant, quantitative domains by 2 separate, blinded reviewers (Cohen’s kappa = 0.99) and multilevel comparisons were performed using Kruskal-Wallis or ANOVA tests, where appropriate.
RESULTS: 197 patients were enrolled – 97 (49.2%) at DRH, 50 (25.4%) at TTCIH, and 50 (25.4%) at UHWI. Mean (SD) age (50.5 [13.1] yrs vs. 51.6 [9.1] yrs vs. 50.8 [10.4] yrs; p=0.86) and gender distribution (% male: 49.5 vs. 44 vs. 40; p=0.53) were similar across sites but patients at DRH were more hypertensive at presentation (mean systolic blood pressure [SD] in mm Hg: 166.8 [28.0] vs. 153 [18.1] vs. 152.7 [27.9]; p=0.003), had a longer mean (SD) duration of cHTN (12.1 [11.0] yrs vs. 4.6 [5.8] yrs vs 9.1 [7.6]; p<0.0001), and were less likely to be on antihypertensive therapy (84.5% vs. 92% vs. 100%, p=0.001). Explanatory models (Table) revealed limited recognition of cHTN as a “disease” (19.6% vs. 28% vs. 16%; p=0.31) and consistency in the belief that cHTN was curable (44.3% vs. 36% vs. 42%; p=0.62). Stress (48.4% vs. 60% vs. 50%; p=0.31) and, especially at DRH, diet (62.2% vs. 22% vs. 36)%; p<0.0001) were identified most frequently as causes of cHTN and an association with symptoms was common (83.5% vs. 98% vs. 78%; p=0.15). Clear differences existed for perceived benefits of treatment and consequences of poor control by site but in general, both were under-appreciated.
CONCLUSIONS: Misperceptions related to cHTN are common in the ED. While specific areas of disconnect exist by geographic region, under-appreciation of cHTN as a dire and fixed disease state is consistent suggesting that a uniform educational intervention may be of benefit in this setting.
Related articles