Abstract
Purpose
Chest wall (CW) toxicity (rib fracture and/or pain) is recognized complication of stereotactic body radiotherapy (SBRT) for non-small cell lung cancer (NSCLC). The aim of this study was to evaluate the frequency of CW toxicity following SBRT and propose a new dosimetric parameter adapted to fractionation.
Materials and Methods
We reviewed the charts and SBRT plans from patients treated for T1-T2N0 peripheral NSCLC between 2009 and 2015. The CW structure was created through a 3 cm expansion of the lung. The median dose delivered to the planning target volume was 60 Gy. SBRT was delivered in 3 fractions for patients with CW V30 of less than 30cc. If the CW V30 exceeded 30cc, 5 fractions were used and the plan was optimized based on the CW V37 (considered biologically equivalent to the V30 of 3 fraction plans).
Results
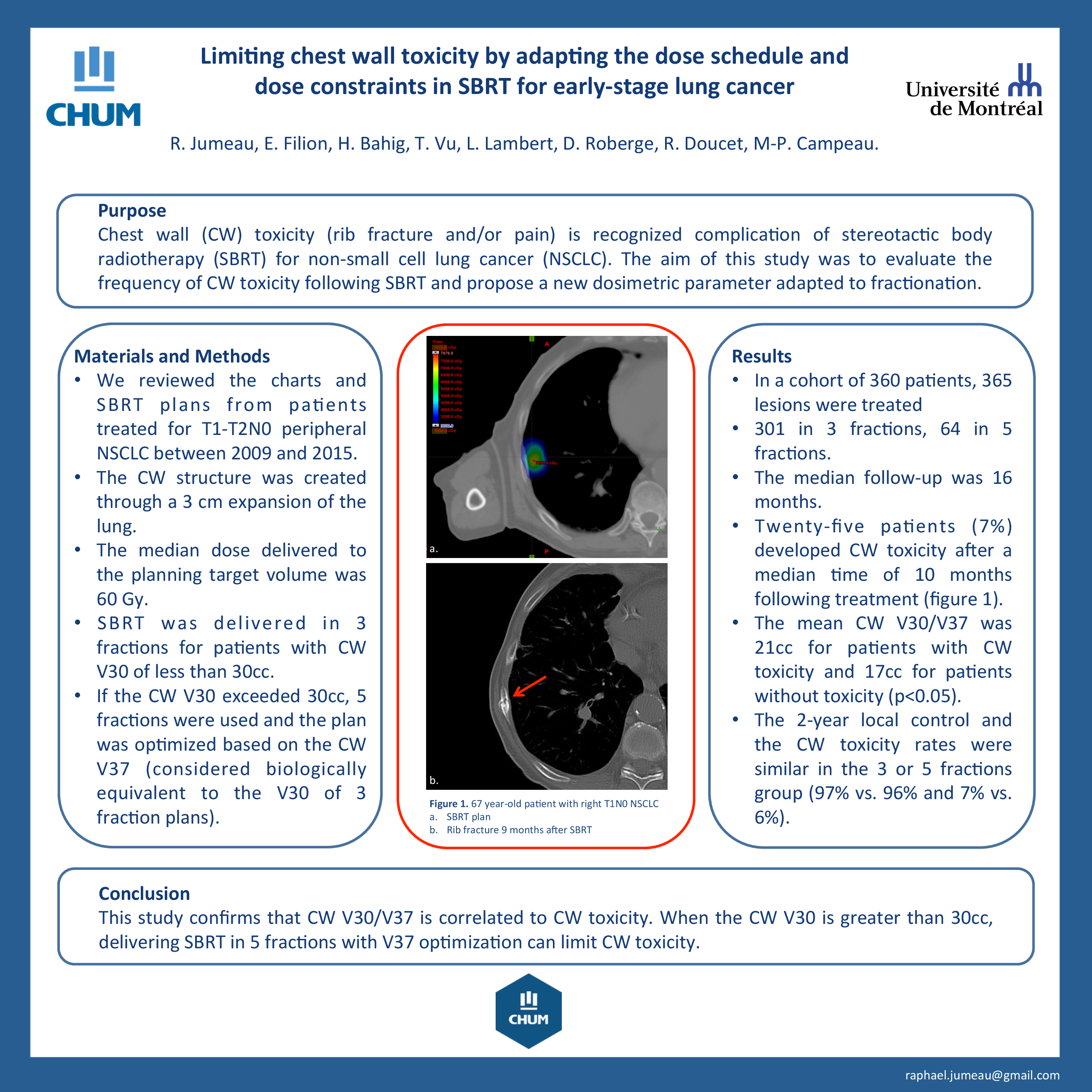
In a cohort of 360 patients, 365 lesions were treated 301 in 3 fractions, 64 in 5 fractions. The median follow-up was 16 months. Twenty-five patients (7%) developed CW toxicity after a median time of 10 months following treatment. The mean CW V30/V37 was 21cc for patients with CW toxicity and 17cc for patients without toxicity (p<0.05). The 2-year local control and the CW toxicity rates were similar in the 3 or 5 fractions group (97% vs. 96% and 7% vs. 6%).
Conclusion
This study confirms that CW V30/V37 is correlated to CW toxicity. When the CW V30 is greater than 30cc, delivering SBRT in 5 fractions with V37 optimization can limit CW toxicity.