Abstract
Objectives: Evidence from multiple non-randomised studies demonstrate that SBRT is associated with very high 1- and 2-year local control rates and can be delivered with minimal toxicity. Guy’s and St Thomas’ academic hospital successfully bid in NHS England’s CtE programme to become one in 17 SBRT centers (for oligometastases) & one of 4 centers in England for HCC and recurrent pelvis treatment. This is a busy public hospital with catchment area of 1.7 million and 7 Linacs and we see 6000 new cancer cases per year.
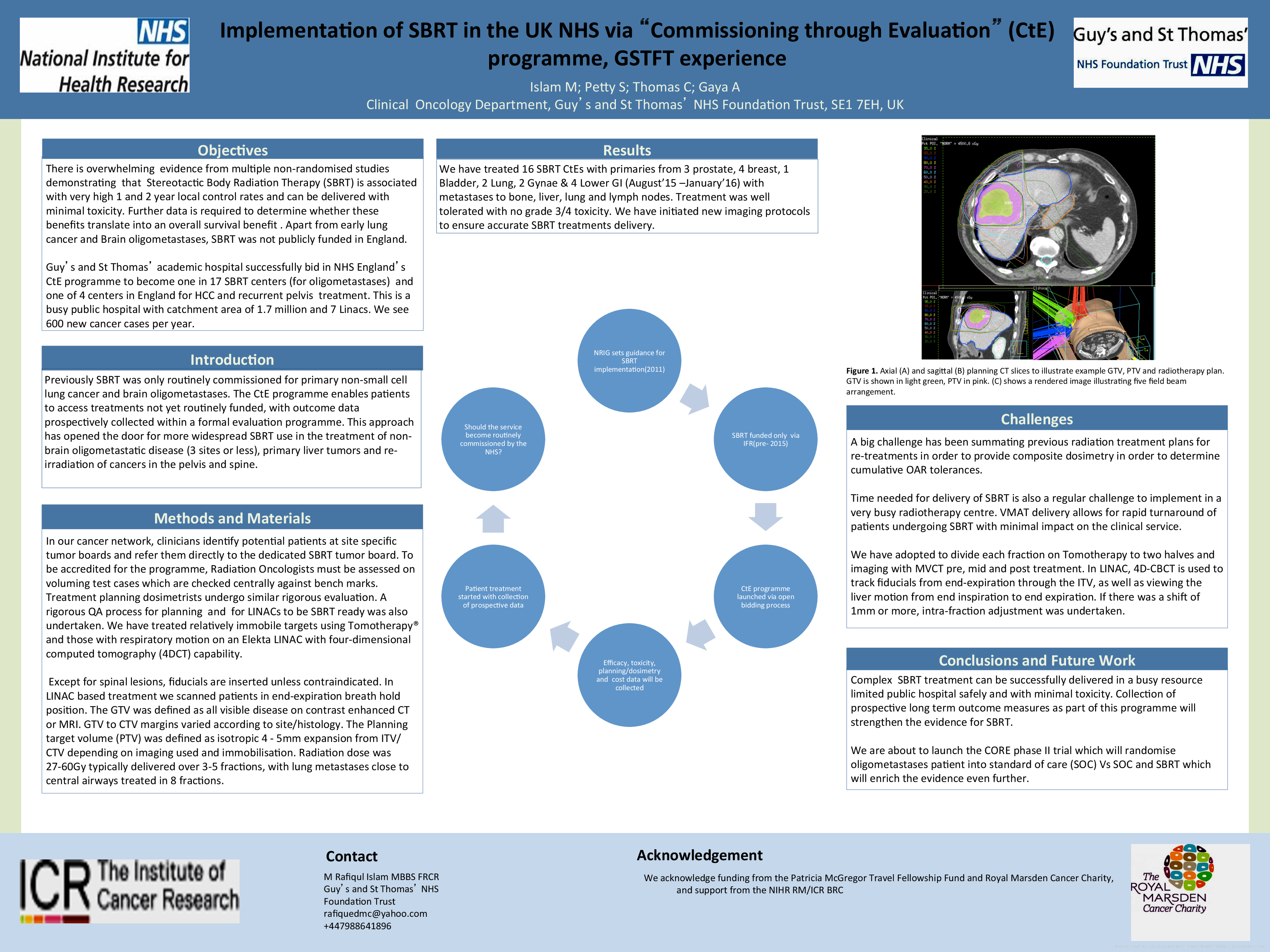
Methods: Previously SBRT was only commissioned for primary NSCLC and brain oligometastases. The CtE programme enables patients to access treatments not yet routinely funded, with outcome data prospectively collected within a formal evaluation programme. This approach allows for more widespread SBRT use in the treatment of non-brain oligometastatic disease (3 sites or less), primary liver tumors and re-irradiation of cancers in the pelvis and spine. Clinicians identify potential patients at site-specific tumor boards and refer them to a dedicated SBRT tumor board. Radiation Oncologists are assessed on voluming test cases which are checked centrally against bench marks. We have treated relatively immobile targets using Tomotherapy® and those with respiratory motion on an Elekta LINAC with four-dimensional computed tomography (4DCT). A rigorous QA process for IMRT planning & for LINACs to be SBRT ready was also undertaken. Except for spinal lesions, fiducials are inserted unless contraindicated. In LINAC based treatment, we scan patients in end-expiration breath hold position. The Gross Tumor volume (GTV) was defined as all visible disease on contrast enhanced CT or MRI. GTV to CTV margins varied according to site/histology. The Planning target volume (PTV) was defined as isotropic 4-5mm expansion from ITV/CTV. Radiation dose was 27-60 Gy typically delivered over 3-5 fractions, with lung metastases close to central airways treated in 8 fractions. A big challenge has been summating previous radiation treatment plans for re-treatments to provide composite dosimetry in order to determine cumulative OAR tolerances. We divide each fraction on Tomotherapy to two halves and imaging with MVCT pre, mid and post treatment. In LINAC, 4D-CBCT is used to track fiducials from end-expiration through the ITV, as well as viewing the liver motion from end inspiration to end expiration. If there was a shift of 1mm or more, intra-fraction adjustment was undertaken. Time needed for delivery of SBRT is also a regular challenge to implement in a very busy radiotherapy centre. VMAT delivery allows for rapid turnaround of patients undergoing SBRT with minimal impact on the clinical service.
Results: We have treated 16 SBRT CtEs with primaries from 3 prostate, 4 breast, 1 bladder, 2 lung, 2 gyn & 4 lower GI with metastases to bone, liver, lung and lymph nodes. Treatment was well tolerated with no grade 3/4 toxicity. We have initiated new imaging protocols to ensure accurate SBRT treatments delivery.
Conclusions: Complex SBRT treatment can be successfully delivered in a busy resource-limited public hospital safely and with minimal toxicity. Collection of prospective long term outcome measures as part of this programme will strengthen the evidence for SBRT. We are about to launch the CORE phase II trial which will randomise oligometastases patient into standard of care (SOC) Vs SOC and SBRT which will enrich the evidence even further.