Abstract
Introduction:
There has been no clinical trial to evaluate the efficacy of acetazolamide treatment for idiopathic intracranial hypertension (IIH). In this prospective study, we used high speed eye movement recording to characterize reflexive saccades in patients with IIH and to assess the effectiveness of acetazolamide.
Methods:
We recorded 25 consecutive patients referred for evaluation of IIH with 500-Hz binocular infrared oculography. Eighten patients fulfilled the Modified Dandy criteria for IIH1,2,3,4, and data from 16 patients with good recordings (10 paired recordings performed before and on acetazolamide) were analyzed. Stimuli included reflexive centrifugal saccades. Each eye was calibrated independently, and data were analyzed with MATLAB and IgorPro.
Results:
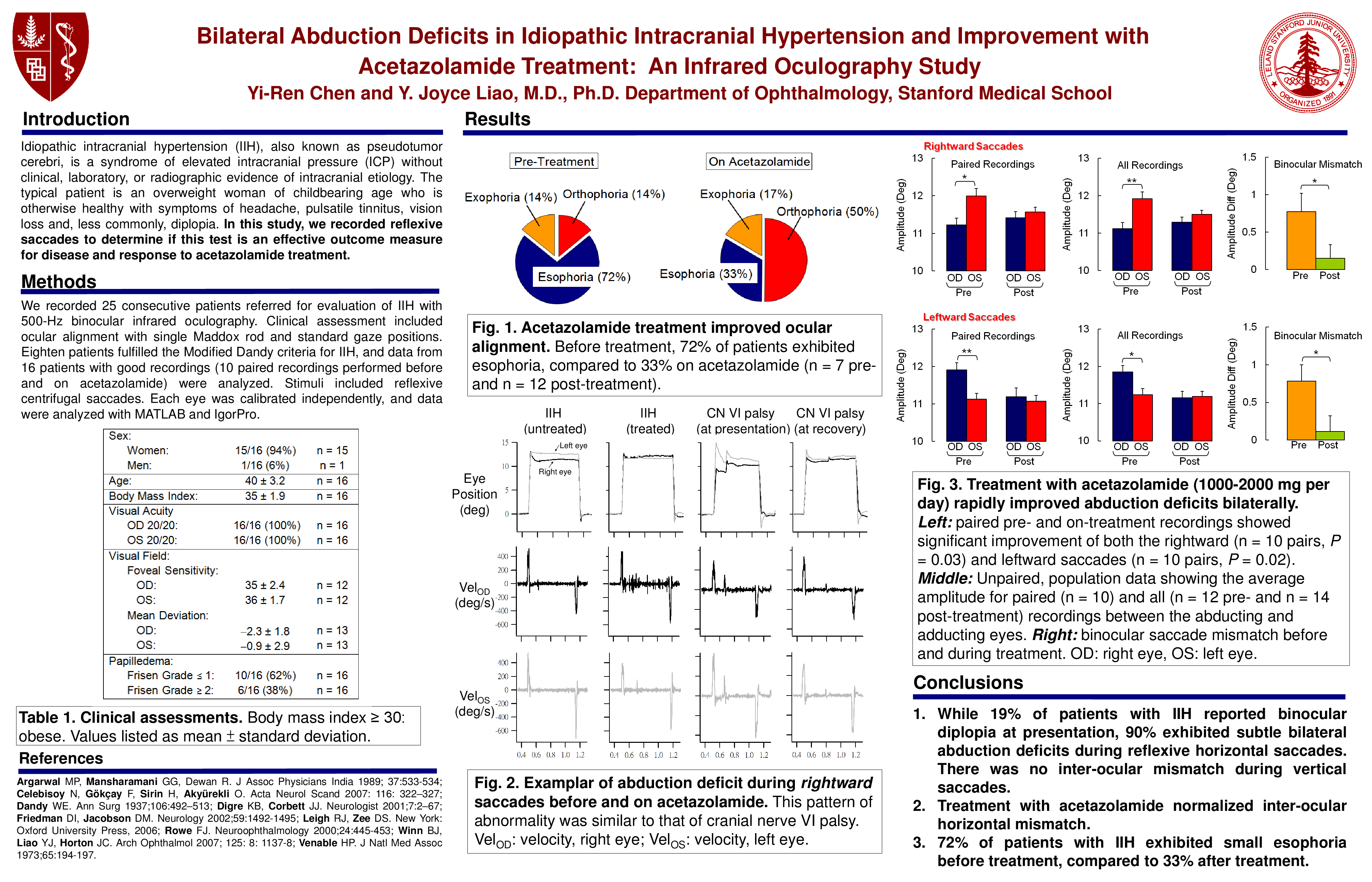
In 16 IIH patients (15 women/1 man, age 39.8±3.2, body mass index 35.4±1.9), symptoms included headache (100%), vision loss (56%), tinnitus (69%), and diplopia (19%). All patients had visual acuity of 20/20 bilaterally, visual field loss grade ≤25, and papilledema. Alignment was 63% orthophoric and 31% esophoric. On infrared oculography, 90% of patients with paired recordings (n=10) had bilateral abduction deficits. In horizontal saccades, plateau amplitude showed 0.8±0.2 deg abduction deficit (center-to-left: OD 11.9 deg, OS 11.1 deg, P=0.006; center-to-right: OD 11.2 deg, OS 12.0 deg, P=0.01). Data from all patients (non-paired) also showed significant bilateral abduction deficits (center-to-left: P=0.02, center-to-right: P=0.005). Despite this abducton deficit in saccade amplitude, there was no difference in peak velocity. There was also no binocular mismatch in vertical saccades (center-to-up: P=1.0; center-to-down: P=0.9). Acetazolamide treatment eliminated this bilateral abduction deficit (center-to-left: P=0.02; center-to-right: P=0.03), with no effects on vertical saccades (center-to-up, P=0.5; center-to-down, P=0.5) or peak velocities in all directions.
Conclusion:
Despite the lack of symptomatic binocular diplopia and cranial nerve VI palsy, 90% of patients with IIH exhibited bilateral abduction deficits during reflexive saccades. This difference disappeared after acetazolamide treatment, along with symptomatic improvement of headache, vision loss, and diplopia.
References:
1 Shah, VA, Kardon, RH, Lee, AG, Corbett, JJ, Wall, M. Long-term follow-up of idiopathic intracranial hypertension: The Iowa experience. Neurology, 70, 634-640, 2008.
2 Friedman, DI, Jacobson, DM. Idiopathic intracranial hypertension. J Neuro-Ophthalmol, 24, 138-145, 2004.
3 Digre, KB, Corbett, JJ. Idiopathic intracranial hypertension (pseudotumor cerebri): a reappraisal. Neurologist, 7, 2-67, 2001.
4 Smith, JL. Whence pseudotumor cerebri? J Clin Neuro Ophthalmol, 5, 55-56, 1985.
5 Rowe, FJ, Sarkies NJ. Assessment of visual function in idiopathic incranial hypertension: a prospective study. Eye, 12, 111-118, 1998.