Abstract
Background: High-fidelity simulation-based education has shown improved resident knowledge and performance1,2,3. While there is evidence that learning is not dependent on simulator fidelity4, there is little research on low-fidelity simulation to teach complex scenarios, particularly in pediatrics. Rapid Cycle Deliberate Practice is a simulation technique allowing for rapid feedback and mastery of skills with graded difficulty levels5. It focuses on initial assessment and initial stabilization steps, which are most likely to be life-saving in a low-resource setting, while traditional debriefing focuses more on advanced skills occurring later in the scenario. We sought to develop a year-long simulation-based curriculum for pediatric residents in Rwanda utilizing instruction with either RCDP or traditional debriefing.
Research Questions: Will a simulation-based curriculum for pediatric residents in Rwanda utilizing instruction with Rapid Cycle Deliberate Practice lead to greater improvement on simulation-based performance when compared with instruction utilizing Traditional Debriefing?
Methodology: Research was approved by the Kigali University Teaching Hospital (KUTH) IRB as well as by the Boston Children’s Hospital and Texas Children’s Hospital IRBs. Pediatric residents rotating at the Kigali University Teaching Hospital (KUTH) were randomly assigned to one of two simulation curriculum groups (RCDP or traditional simulation) and completed a six month-long simulation-based curriculum designed to improve pediatric resuscitation skills. Cases addressed management of shock, respiratory failure, and cardiac arrest.
Basic demographic data and data regarding previous training were collected. Residents were tested on their performance on a simulation-based based pediatric resuscitation before and after the curriculum. Pre- and post- simulation tests were videotaped and reviewed by 2 of the investigators using a modified version of the Simulation Team Assessment Tool with the blinded investigator’s scores used for data analysis, and the non-blinded investigator’s scores used to calculate the intraclass correlation coefficient (ICC).
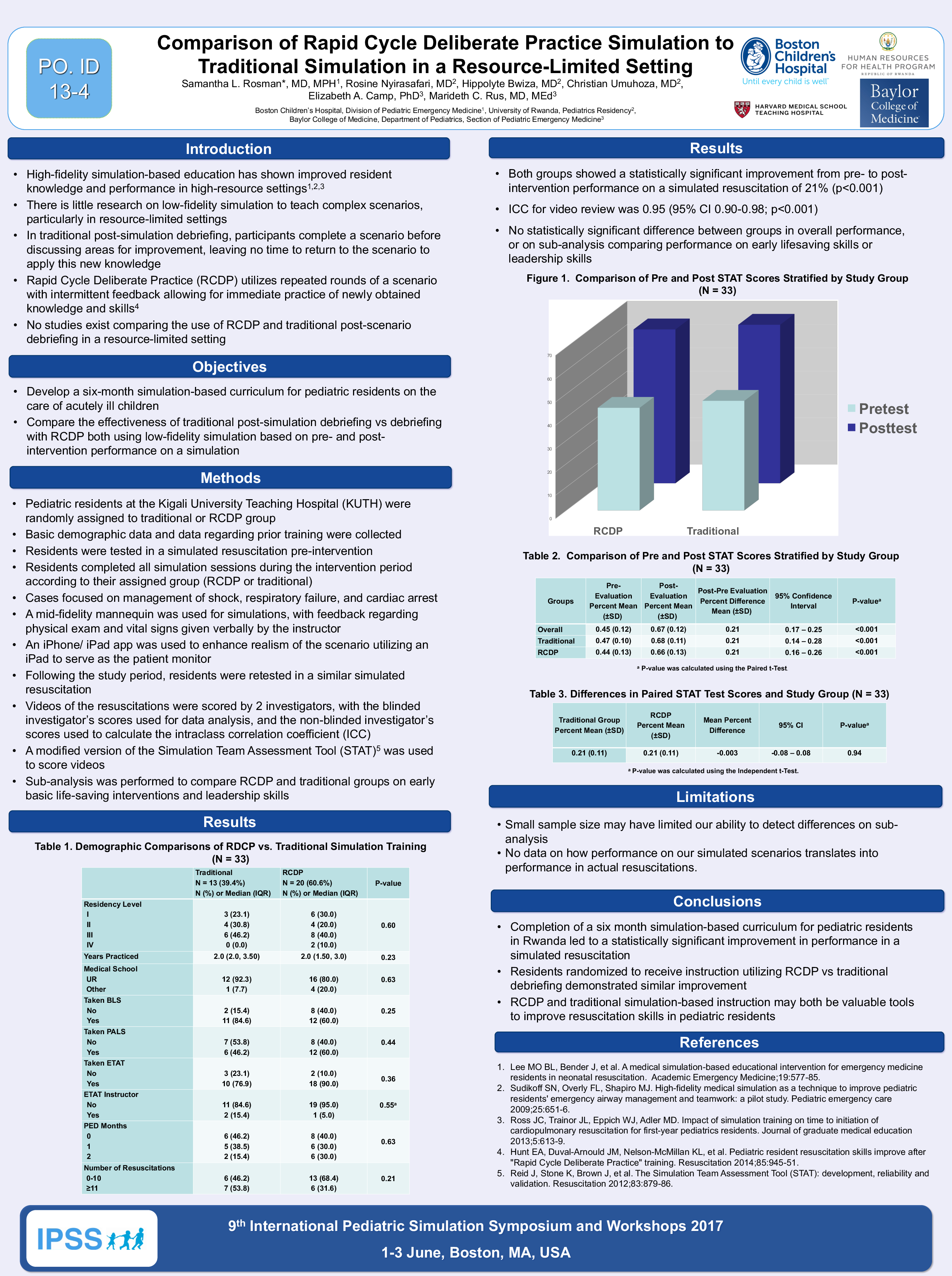
Results: There were no significant differences in the demographic factors between the groups randomized to RCDP and traditional. Pre-test scores on the simulated resuscitation for the overall group, RCDP group, and traditional group were 45%, 44% and 47% respectively. Post-test scores for the overall group, RCDP group, and traditional group were 67%, 66%, and 68%, demonstrating a statistically significant mean improvement of 21% in each group (p<0.001). There was no statistically significant difference between the RCDP and traditional groups in overall performance, or on sub-analysis comparing performance on early lifesaving skills or leadership skills. The ICC for video review was 0.95 (95% CI 0.90-0.98; p<0.001)
Discussion/Conclusions: Completion of a six month simulation-based curriculum for pediatric residents in Rwanda led to statistically significant improvement in performance in a simulated resuscitation. Residents randomized to receive instruction utilizing RCDP vs traditional debriefing demonstrated similar improvement. RCDP and traditional simulation-based instruction may both be valuable tools to improve resuscitation skills in pediatric residents in limited-resource settings.