Abstract
Objectives: Phase 2 SBRT studies have shown that pts w/ =3 metastases have better PFS & overall survival (OS) than pts w/more widespread disease, & breast cancer pts may fare best. High rates of local control are seen, together w/cceptable rates of toxicity for oligomes. PFSrates in these studies are better than would usually be expected in stage 4 disease; however, lack of randomized data limits interpretation. Control group is required to evaluate true benefit of adding SBRT to systemic tx & which pt groups are most likely to benefit. Potential therapeutic benefit of adding SBRT to standard therapy may vary between tumor sites, reflecting the different underlying tumor biologies, immunology & natural disease course.
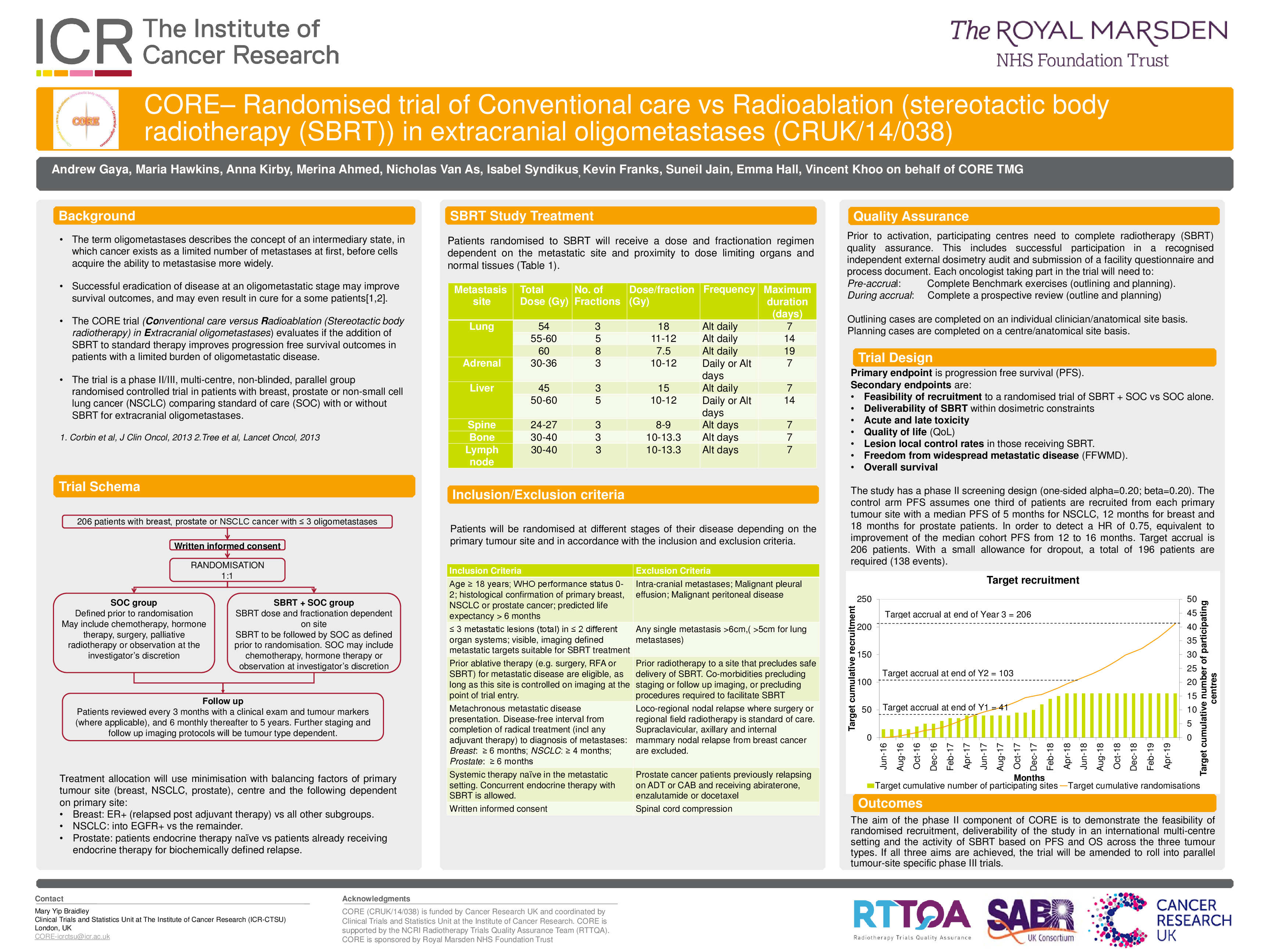
Methods: CORE (CRUK/14/038) is a phase II/III, multi-centre, non-blinded, parallel group randomised controlled trial in pts w/breast, prostate or NSCLC cancer comparing SOC w/wo SBRT for extra-cranial mets. 206 pts for phase II trial; Eligible pts: w/either primary breast, prostate or NSCLC presented w/ =3 extra-cranial metachronous oligometastases, all suitable for SBRT. Max of 2 different organ systems may contain mets, total # lesions not >3. No prior tx for metastatic disease, & =6 months DFI breast & prostate pts; =4 months NSCLC from completion of primary radical tx. Main exclusion criteria include IC mets, malignant pleural effusion or peritoneal disease, a met >6cm (>5cm lung), & prior RT to site that precludes safe delivery of SBRT. Pts randomised (1:1 ratio) to SOC alone or SOC & SBRT. Choice of SOC at discretion of treating oncologist & defined per pt prior to randomisation. It may include any standard therapy that is clinically appropriate e.g. chemotherapy, biological therapy, endocrine therapy, palliative radiotherapy or observation. Pts randomised to SBRT will receive dose & fx regimen dependent on met site & proximity to dose limiting organs & normal tissues. Staging & fu imaging protocols tumor type dependent.
Results: Primary endpoint to evaluate if the addition of SBRT to SOC improves PFS in pts w/limited burden of oligometastatic disease. Secondary endpoints include the dose level achievable within the dosimetric constraints, evaluation whether the addition of SBRT to SOC improves OS, lesion local control rates in those receiving SBRT, acute & late toxicity associated w/the addition of SBRT to SOC, & QOL in pts receiving SBRT compared to those receiving SOC alone. Study will also evaluate if the addition of SBRT to SOC improves freedom from widespread metastatic disease (FFWMD).
Conclusions: The aim of the CORE phase II is to demonstrate (1) feasibility of randomised recruitment, (2) deliverability of the study in an int'l multi-centre setting & (3) the activity of SBRT based on PFS & OS across 3 tumor types. If all 3 aims achieved trial will be amended to roll into parallel tumour-site specific phase III trials.